By local growth sclerosing orbital pseudotumors can cause bulging of the eye (proptosis).
Sclerosing orbital pseudotumor is uncommon. Due to unknown reasons, these tumor behave differently than other types of pseudotumor of the orbit. They grow more slowly, cause less pain, and are characterized by scarring (hardening of the tumor tissue).
Symptoms
Sclerosing orbital pseudotumor is not cancer. But, by local growth it can cause bulging of the eye (proptosis), double vision (diplopia) and loss of vision. Sclerosing orbital pseudotumor can (rarely) extend into the sinuses, brain, and other orbit.
Diagnosis
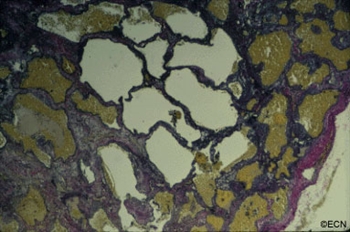
Histopathology reveals large amounts of fibrous tissue.
Sclerosing orbital pseudotumor is usually diagnosed by biospy (orbitotomy).
Once the diagnosis is confirmed by pathology, systemic testing to rule out specific infectious and inflammatory causes should be performed. For example, an ANCA blood test and a chest x-ray should be performed to rule out Wegener’s Granulomatosis. Many of these patients have a past medical history of sinusitis, sinus surgery, or inhalation drug abuse. Therefore, concurrent treatable sinus disease should be addressed.
Treatments
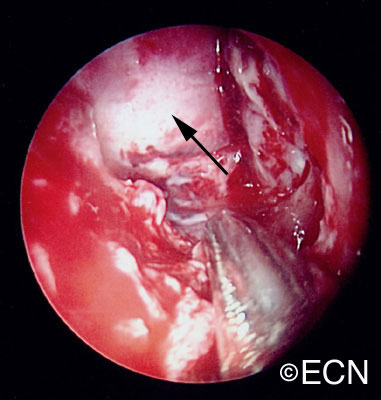
In this case, computed tomographic (CT) scanning demonstrates a mass in the nasal orbit. The arrow demonstrates the optic nerve on stretch. The eye wall (sclera) is indented and the eye pushed out (proptosis).
Sclerosing orbital pseudotumors are less responsive to steroid therapy. Most cases are treated with combinations of surgery, steroid therapy, radiation and chemotherapy depending upon the clinical picture and the patient’s response to treatment.
Inflammations can affect the tissues around the eye (orbit and adnexa). Certain orbital inflammations can look like tumors and are therefore called orbital pseudotumor. Orbital pseudotumor can affect one or both eyes of relatively young patients (less than 50 years old). They are not cancer.
Symptoms
Orbital pseudotumor can be quite painful. In fact, pain is one of the most prominent characteristics of this disease. In addition to pain, an inflammatory mass (tumor) can make the patient’s eye protrude (proptosis) and restrict the movement of the eye. A biopsy (called an orbitotomy) is commonly performed to confirm the diagnosis of orbital pseudotumor and to obtain tissue for pathology examination.
Diagnosis
Orbital pseudotumor is typically characterized by the rapid development of pain, proptosis, and swelling around the eye and orbit in adults. Ultrasound and computed tomographic (CT) scanning typically shows a diffuse infiltration of the orbit, an inflammation of the eye wall (sclera), and/or T-sign (with the optic nerve). Orbital pseudotumor related orbital masses typically have poorly defined margins. Systemic testing (blood and spinal fluid) may show signs of inflammation (e.g. increased sedimentation-rate) or atypical cells.
Patients with classic findings of orbital pseudotumor may be treated without a biopsy. A rapid complete response to steroid therapy helps confirm the diagnosis. Atypical cases of orbital pseudotumor usually undergo a diagnostic biopsy.
Specimens can be sent to test for infectious causes of orbital inflammation and certain systemic diseases. Typically eye cancer specialists will obtain blood, skin and radiographic (e.g. x-ray, MRI) tests for a variety of diseases such as sarcoidosis, tuberculosis, and Wegener’s Granulomatosis (see table below). An orbital biopsy can be particularly helpful in diagnosing many of these disorders.
Treatments
Orbital pseudotumor will respond rapidly to high-dose steroid therapy. Unfortunately, when the steroids are stopped, the inflammation often returns. Eye cancer specialists must reduce the steroid medication very slowly in order to prevent recurrence (return) of the disease.
In certain cases, chemotherapy (e.g. methotrexate, cyclosporine) and low-dose radiation (e.g. 1500-2500 cGy EBRT) may be needed to control the inflammation related to orbital pseudotumor. Most patients do well with steroid therapy but they are always at risk for recurrent orbital pseudotumor.
Additional info
Other Common Causes of Orbital Swelling and Inflammation:
Color Photographs: Juxtapapillary Capillary Hemangioma
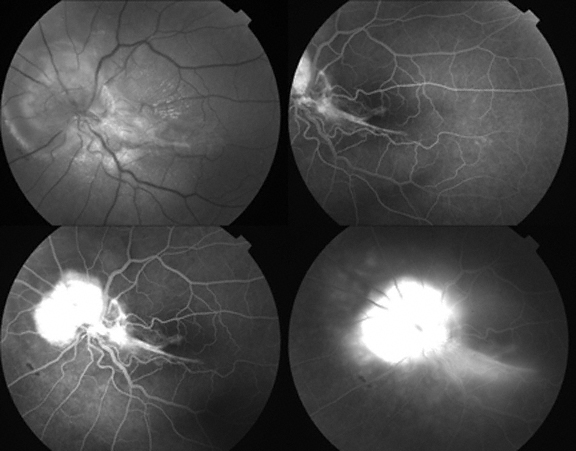
Dr. Soarnil would appreciate suggestions as to treatment options to optimize visual outcome without risk to this 42 year old woman with a juxtapapillary hemangioma.
“This is a case of juxtapapillary capillary hemangioma in a patient with V-H-L Disease, a woman 42 yo. She came to my clinic in February 2007, presenting a VA 20/20 in both eyes, no capillary hemangiomas in the RE and a juxtapapillary hemangioma in the left eye, asymptomatic. After 6 months, she started having visual symptoms and exudates (Top) and we performed TTT treatment. Exudates decreased, but an epiretinal membrane appeared. Hemangioma activity persisted, and a second TTT was performed December 2007, and ERM symptoms worsened and the hemangioma persisted.
View the fluorescein angiogram taken after TTT – treatment
Flourescein Angiography of the juxtapapillary hemangioma
What do you think is the next step? Intravitreal injection of anti- VEGF? Vitreoretinal surgery with endophotocoagulation ? Brachytherapy? Any combination? I will appreciate very much your suggestions.
These magnetic resonance imaging (MRI) studies demonstrate displacement of the optic nerve, a bright T1 tumor image, and a variably bright T2 tumor image. The tumor is noted to involve the orbit, the ethmoid and frontal sinuses.
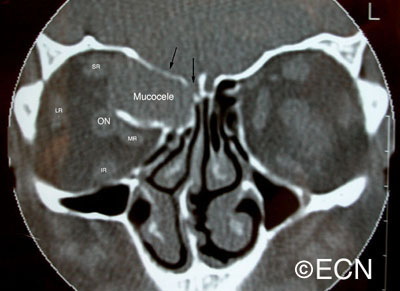
Orbital mucocele can occur when sinus mucoceles cannot naturally drain through the nose. Instead, they grow and slowly invade adjacent orbital tissues.
Generally arising from the ethmoid or frontal sinuses, orbital mucoceles are mucous or fluid filled cysts which can displace the eye. Frontal sinus mucoceles can force the eye down, ethmoid tumors will push the eye out and maxillary lesions can elevate or push the eye in. Lastly, orbital mucoceles originating in the sphenoid sinus can compress the optic nerve resulting in loss of vision.
Symptoms
Patients with mucocele of the orbit, typically have a history of facial trauma or chronic sinus disease. They tend to be in their mid 40’s or older. They can have painless proptosis, or complain of headaches, double vision, or loss of vision.
Diagnosis
Computed axial tomography demonstrates displacement of the medial rectus muscle (MR), as well as erosion and obliteration of portions of the orbital roof (black arrows). Note that the orbital portion of the mucocele is partially encased in bone. This is characteristic of mucocele. The rectus muscles and optic nerve are labeled.
demonstrates displacement of the medial rectus muscle (MR), as well as erosion and obliteration of portions of the orbital roof (black arrows). Note that the orbital portion of the mucocele is partially encased in bone. This is characteristic of mucocele. The rectus muscles and optic nerve are labeled.
Though magnetic resonance imaging (MRI) can be consistent with a mucous or serous fluid-filled tumor, a drainage procedure is typically required and found to be diagnostic. The mucoid or serous fluid (which is found to make up the mucocele) should be sent for culture and sensitivity as well as cytologic examination. Mucoceles can be infected. In those cases, the choice of antibiotics can depend on cultures taken during surgery.
Treatments
Intraoperative transnasal video photography is presented to show the mucocele cavity (arrow) after ethmoidectomy (photograph courtesy of Steven Schaefer, MD)
The treament of mucocele of the orbit is surgical. It is best to have a combination of an ophthalmic and ENT surgeons. Treatment involves removal of as much of the cyst and its lining as possible. This usually requires an orbitotomy and sinusectomy. It is most important to re-establish or create a new drainage pathway for the mucous to exit the nose.
Additional info
Case Example: A 63 year old male was referred to The New York Eye Cancer Center with a 6 month history of progressive painless proptosis of the right eye.
Despite this large orbital tumor with optic nerve displacement, the patient was 20/20 OU, he had no visual field defect, and no signs of optic neuropathy. A complete medical survey was initiated and the patient was cleared for surgery. A combination of anterior orbitotomy and transnasal ethmoidectomy were performed to evacuate the mucous and allow for future drainage.
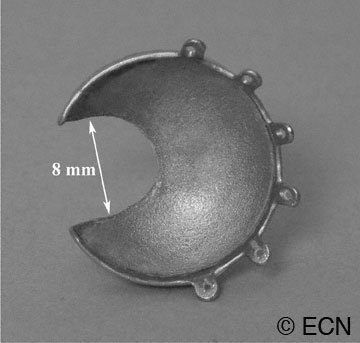
Dr. Finger invented “Slotted Eye Plaques” for treatment of juxtapapillary and circumpapillary intraocular tumors. Standard COMS-type gold eye-plaques were altered such that an 8-mm-wide (variable length) slot was created to accommodate the orbital portion of the optic nerve. As the nerve entered the slot, the plaque’s posterior margin extended beyond the optic disk as to cover tumor (on the opposite side). Radioactive seeds around the slot, surround the tumor and its posterior tumor margins.
Dr. Finger says, “due to the physical limitations of notched plaques, there was no plaque device that could extend to cover and treat the posterior portion of a tumor that came within 1.5 mm, touched or surrounded the optic nerve.” This is why Dr. Finger invented slotted eye plaques. Intraoperative ultrasound imaging is used to confirm proper plaque placement. Preoperative radiation dosimetry showed that all tumour-tissue received a minimum of 85Gy (despite the gap created by the slot). To date, there has been only one tumor regrowth which is much better than previous plaque treatments for these tumors. No new complications that might prevent the use of slotted plaque radiation therapy have been noted.
Graphic Animation of a Slotted Plaque in Position over a Circumpapillary Tumor
Dr. Finger says, “slotted plaques represent an innovation that improves radiation coverage for tumors that touch or surround the optic nerve. For the first time, this technique allows plaque radiation therapy to include the entire juxtapapillary and circumpapillary tumor within the treated zone. It “normalizes” plaque treatment of these tumors. He adds, this technique addresses the problems some centers were having with local control of tumors in this location. Certainly, it will allow more patients to keep their eyes and their vision.”
For more complete information read these manuscripts published in the British Journal of Ophthalmology and Ophthalmology in 2012 or contact Dr. Finger.
Graphic of how an eye can look with a posterior orbital tumor.
Orbital and optic nerve meningioma can extend from the brain into the orbit (behind the eye) and push the eye forward causing a bulging of the eye called proptosis. Though rare, when they occur, they are a significant cause of vision loss.
Symptoms
Patient with orbital meningioma typically have proptosis (bulging eye). Optic nerve compression can cause optociliary shunt vessels to form, as well as loss of vision. Depending on the location, size and degree of optic nerve involvement; patients can develop monocular and/or junctional defect is the patients field of vision.
Diagnosis
Opto-ciliary shunt vessels resulting from optic nerve compression
Patients usually present in their 40s and may have neurofibromatosis type 2. In making this diagnosis, one should look for the triad of vision loss, optic atrophy and abnormal vessels on the optic nerve. The nerve head can appear raised. Enlarged blood vessels are called “optociliary shunt vessels” and indicated that the meningioma has disrupted the natural circulation through the optic nerve to the retina and choroid. Angiography of the optic nerve head will clearly demonstrate the abnormal blood vessels. Magnetic resonance imaging (MRI), ultrasonography and computed tomographic (CT) imaging have been used to evaluate the orbital tumor and measure the optic nerve sheath diameter. CT is particularly helpful for imaging calcium within the tumor.
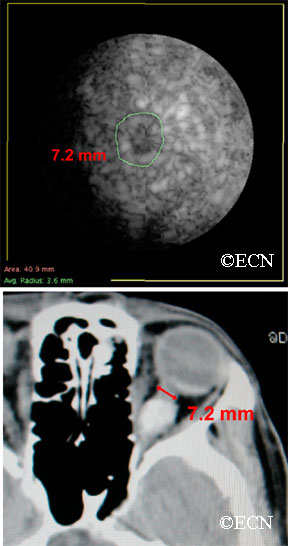
Computed tomography (CT) shows that the eye is pushed forward by this optic nerve sheath meningioma. Notice that the tumor is relatively bright (radio-dense). Imaging of the brain can determine if the meningioma extends into the brain.
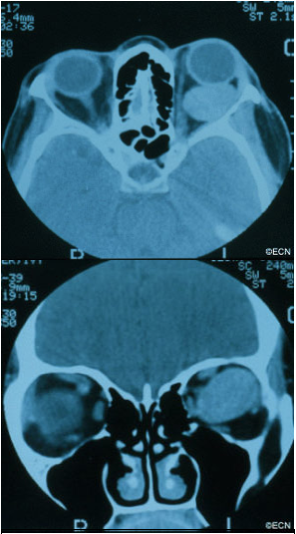
In the images above, note that computed tomography of this optic nerve sheath meningioma. C demonstrates the calcific density of the left optic nerve. An x-ray film shows the linear density (seen on the right side of the film crossing the inferior orbital rim) which corresponds to the optic nerve sheath meningioma seen above.
Coronal “C-scan” ultrasound can be used to compare optic nerve diameters in a case of optic nerve sheath meningioma
Treatment Plan
Orbital meningioma is typically a slow-growing tumor. Once diagnosed, meningioma can be observed for growth prior to considering intervention. Treatment is indicated when there is a risk of spread to the central nervous system (in primary optic nerve sheath meningioma), documented progressive vision loss, or for rapid growth.
Computed tomography of the optic nerve sheath meningioma. Note the almost calcific density of the left optic nerve. An x-ray film shows the linear density (seen on the right side of the film crossing the inferior orbital rim) which corresponds to the optic nerve sheath meningioma seen above.
Though microsurgical resections have been tried (in an effort to spare the optic nerve), most eventually fail. The goal of local resection should be complete removal of the meningioma. This usually involves removal of the involved optic nerve. If complete surgical removal is not possible or in special circumstances, radiation therapy is commonly employed.
Biopsy:
Indications for biopsy include: atypical tumors, aggressive disease, acute vision loss and when a pathology diagnosis is requested. Certain inflammatory tumors can have a similar appearance to orbital meningiomas. However, biopsy carries risk for vision loss.
Treatment:
Orbital meningioma is typically a slow-growing tumor. One must consider patient age, rate of tumor growth and risk for loss of vision. That said, once diagnosed slow or non-growing meningiomas can be observed for further growth or stabilization prior to considering intervention. In general, treatment is indicated when there is a risk of spread to the central nervous system (in primary optic nerve sheath meningioma), documented progressive vision loss, or for rapid growth.
Treatment alternatives are tailored to the clinical situation. For example, if vision is lost, the tumor is growing toward the central nervous system and is resectable; it is removed. If complete surgical removal is not possible or in special circumstances,microsurgical resection or external beam radiation therapy can be considered. These decisions are complex and best made with your neuro-ophthalmologist, neurologist and orbital surgeon.
Computed Tomography (CT) shows a large lymphangioma (arrow), pushing the eye out of the orbit.
Description
Lymphangioma is rare (less than 7% of childhood orbital tumors). Patients can present with acute proptosis (bulging eye) after minor head trauma, as a gradual proptosis, or after an upper respiratory infection.
Symptoms
Lymphangioma tends to start in the superior and nasal orbital quadrants. More than 50% affect anterior (conjunctival and adnexal) structures. Typically, the lymphangioma bleeds into itself causing cysts of blood (called chocolate-cysts) within the tumor. If the cyst forms behind the eye, it pushes the eye forward. If the tumor forms in the eyelid or structures around the eye “adnexa”, blood filled lymphatic channels called “lymphangiectasias” can be seen beneath the conjunctiva
Diagnosis
A lymphangiectasia is seen beneath the conjunctival surface.
Lymphangioma is usually diagnosed by an eye cancer specialist. A careful history may reveal sudden painful proptosis (bulging of the eye), facial trauma or that the tumor or proptosis started right after a upper respiratory infection.
Physical examination may reveal bluish discoloration of or blood vessels within the eyelid skin. Should the vessels extend under the conjunctiva, they are called lymphangiectasias.
Severe cases can be associated with corneal exposure, ulceration and optic nerve damage.
Treatments
Though lymphangioma patients can present with a history of sudden proptosis (due to bleeding within the tumor), orbital lymphangiomas are typically slow growing. Therefore, most lymphangiomas are followed by observation for growth-related damage as documented by (clinical and radiographic studies) prior to intervention.
Thus, treatment of lymphangioma is indicated when associated with growth, optic nerve compression, corneal exposure problems (keratitis sicca), glaucoma or vision loss.
When treatment of lymphangioma is considered, the goal is rarely complete removal. This is because the edges of most orbital lymphangiomas are poorly defined. When necessary, patients undergo debulking surgeries with a goal of relieving acute optic nerve compression or corneal exposure. In rare cases, orbital lymphangioma patients may require orbital radiation therapy or exenteration for relief of pain.
Computed tomography (CT) – Coronal Section demonstrates displacement of the optic nerve (medially) by the orbital hemangioma.
Hemangioma is a benign tumor that is found to grow within the orbit. Most commonly located behind the eye globe, it can push the eye forward causing eye-bulging doctors call proptosis.
Symptoms
Cavernous hemangioma of the orbit is most commonly seen in middle-aged women. Most are found within the muscle cone, but can be found anywhere in the orbit.
These orbital tumors can indent the back of the eye causing choroidal folds, or push on the optic nerve causing damage (atrophy).
Rarely, the tumor can push the eye so far that the cornea cannot be covered by the eye lids. In these cases, corneal exposure problems (keratitis, superficial punctate keratopathy, ulceration, even perforation) can occur.
Diagnosis
Cavernous hemangioma of the orbit is usually a slow-growing tumor. If the tumor has not damaged the eye, cavernous hemangioma can be observed for growth prior to considering intervention. Should tumor growth occur, it will be measured by eye examinations including (but not limited to) visual acuity, color vision assessment, Hertel exophthalmometry (a measure for proptosis), as well as an evaluation for double vision (strabismus), corneal exposure, retinal damage, vascular damage, and optic neuropathy.
Treatment
Treatment of orbital hemangioma is indicated when there is evidence of growth, optic nerve compression, and corneal exposure (with secondary keratitis sicca), or evidence of vision loss.
The goal of orbitotomy for choroidal hemangioma should be complete removal of the tumor. This usually involves careful dissection of the tumor to protect the tumor’s capsule (as possible). Connecting vascular feeder vessels should be identified and cauterized. A lateral orbitotomy can be required to keep the large tumor intact.
A fundus photograph demonstrates choroidal folds induced by the choroidal hemangioma indenting the posterior eye-wall.Histopathologic sections with elastin-stain also demonstrate the large loosely distributed vascular channels associated with orbital hemangioma. The tumor’s capsule is noted on the right.
Computed Radiographic Tomography (CT) demonstrates and Adenoid Cystic Carcinoma of the Lacrimal Gland with Orbital Extension (arrow)
Adenoid cystic carcinoma is a type of cancer that affects glandular structures. Around the eye there is a lacrimal (lac-kree-mall) gland that makes tears. Orbital adenoid cystic carcinoma usually occurs in patients 20-50 years old.
Symptoms
When an adenoid cystic carcinoma of the lacrimal gland grows, it typically pushes the eye down, towards the nose and forward. It can cause bulging of the eye (called proptosis). Another characteristic of adenoid cystic carcinoma is that it also invades local nerves causing pain. Therefore, pain and bulging of the eye are the most common symptoms of adenoid cystic carcinoma of the lacrimal gland.
Diagnosis
A complete eye examination with a clinical history and ophthalmic examination are crucial to the diagnosis of adenoid cystic carcinoma of the lacrimal gland and orbit.
CAT scans, MRI’s and ultrasounds are also helpful in determining the diagnosis. When the eye cancer specialist sees a well-defined tumor in the superior-temporal (upper – outer) part of the orbit, that may have eroded into adjacent bone and/or extend into the orbital apex, he or she should suspect the tumor might be an adenoid cystic carcinoma.
Other tumors to consider include: benign mixed tumor, adenocarcinoma, dacryoadenitis, or other processes affecting the lacrimal gland. Often times a biopsy is need to confirm the clinical diagnosis.
Treatments
When possible, an adenoid cystic carcinoma should be totally removed. This usually requires a surgery called a lateral orbitotomy. Unfortunately, total removal is often impossible due to the tumor’s size, shape, and presence of invasion. Should the adenoid cystic carcinoma be found to have a capsule, and should your doctor be able to remove it within its “capsule,” total excisional surgery offers the best prognosis.
However, in many cases the adenoid cystic carcinoma extends beyond the capsule making removal of the entire adenoid cystic carcinoma nearly impossible. It may require removal of the orbital contents, bones and adjacent structures. Due to the poor (local control) results from this type of extensive surgery; combinations of surgical removal, regional chemotherapy and local radiation therapy may be offered as an alternative.
Tumors and inflammations can occur behind the eye. They often push the eye forward causing a bulging of the eye called proptosis.
Tumors and inflammations can occur behind and around the eye. They can push the eye forward causing a bulging of the eye called proptosis (image). Alternatively, if the bulging does not allow the eye lids to close, orbital tumor proptosis can cause corneal breakdown. The most common causes of proptosis are thyroid eye disease and lymphoid tumors (lymphoma and atypical lymphoid hyperplasia).
Other tumors include vascular tumors (e.g. hemangiomas, lymphangioma, hemangiopericytoma), lacrimal gland tumors (e.g. dacryoadenitis, benign mixed tumor, sarcoidosis and adenoid cystic carcinoma), and growths that extend from the sinuses into the orbit (e.g. squamous carcinoma, mucocele). Metastatic cancercan come from other parts of the body to form an orbital tumor. Lastly, an orbit tumor can also be caused by inflammation (e.g. pseudotumor, sarcoidosis) or infection (abscess).
Symptoms
Most patients with orbital tumors notice a bulging of the eyeball or double vision (diplopia). Infections, inflammations and certain orbital cancers can cause pain. Less commonly, orbital tumors are accidentally discovered when patients have a CT or MRI of the head, sinuses and orbit.
Diagnosis
Though CT, MRI’s and ultrasound can help in determining the probable “clinical” diagnosis, most orbital tumors are diagnosed by a surgical biopsy called an orbitotomy (anterior or lateral). During biopsy a specimen is sent to an ophthalmic pathologist who helps determine the exact diagnosis. Dr. Finger has developed a small incision method of orbital biopsy called “FACT.”
Treatments
When possible, orbital tumors are totally removed. If they cannot be removed or if removal will cause too much damage to other important structures around the eye, a piece of tumor may be removed, sent for evaluation by a pathologist and the patient is treated with radiation and/or chemotherapy. Occasionally an orbital tumor is too big or involves the sinuses and requires more extensive surgery with bone-flaps.
If tumors cannot be removed during surgery, most orbital tumors can be treated with external beam radiation therapy. Certain rare orbital tumors require removal of the eye and orbital contents. However, in select cases alternative therapies (e.g. orbital radiotherapy and chemotherapy) can be used to treat residual tumor to spare vision and the eye.
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.