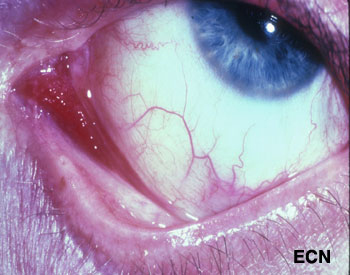
Slit-lamp photograph of a Kaposi’s sarcoma affecting the medial aspect of the conjunctiva into the fornix (arrow).
Kaposi’s sarcoma (KS) can affect the conjunctiva and eyelids. It is a red to pink conjunctival tumor and a blue to purple eyelid tumor. In North America, it is typically found in patients with HIV acquired immunodeficiency syndrome (AIDS), but can occur in the elderly and immunocompromised (e.g. transplant patients). Classic Kaposi’s sarcoma also occurs in the elderly and is slowly progressive.
Diagnosis
If the doctor suspects that a conjunctival tumor is Kaposi’s sarcoma, the patient’s skin and lymph nodes should be examined. Blood should be tested for HIV, lymphocytes, and other opportunistic diseases. One can make a tissue diagnosis based on a biopsy, or a presumptive diagnosis in patients with a history of Kaposi’s. One problem with a presumptive diagnosis (in this group of patients) is that these patients are particularly vulnerable to developing squamous and lymphoid conjunctival tumors.
Your eye care professional is more likely to suggest an incisional biopsy for diagnosis. In most cases, this can be performed in a treatment room with local anesthetic. Sterile technique, HIV precautions, and proper labeling of the specimen are required. In order to biopsy, it is not necessary to completely excise the Kaposi’s sarcoma (unless it is small and unifocal).
Treatments
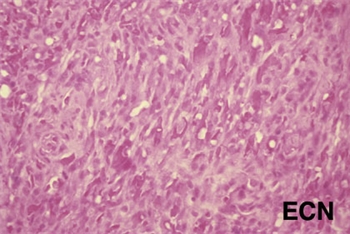
Histopathology of the excised Kaposi’s sarcoma reveals myriads of vascular channels.
Treatment depends on the patient’s age, and the status of his or her general health, current medications and immune status. Small Kaposi’s sarcomas can be removed at biopsy. Larger and multifocal tumors are biopsied, proven Kaposi’s sarcoma by pathologic analysis, and treated (systemically or regionally).
Chemotherapy, radiation therapy and biologic therapy can be employed. In cases of HIV-AIDS related Kaposi’s sarcoma, we tend to avoid any treatment that would further suppress the patient’s immune system. If treatment of the patient’s underlying HIV-AIDS does not halt the progression of the Kaposi’s sarcoma, this tumor has been found to be very sensitive to external beam radiation therapy.
Additional Info
For the ophthalmologist who discovers conjunctival Kaposi’s sarcoma, it is important to coordinate care with a team consisting of a medical oncologist (and/or HIV-specialist), and radiation oncologist.
Malignant cancers can grow on the surface of the eye. They usually start from the membrane that covers most of the eye called the conjunctiva. The most common conjunctival cancers are squamous carcinoma, malignant melanoma and lymphoma.
Malignant melanoma used to be called PAM with atypia, but the newest AJCC staging system authors suggest we stop using the term PAM with atypia and call it melanoma in situ. This was because PAM with atypia doesn’t define it as a cancer. Pathologists call these specimens Tumor in situ or Tis.
Squamous carcinoma of the conjunctiva can form a nodule or diffusely spread out over the surface of the eye. Only very large squamous conjunctival cancers and those in patients who are immunosuppressed metastasize to other parts of the body. But they can invade into and around the eye, into the orbit and sinuses.
Malignant melanoma can start as a conjunctival nevus, arise as newly formed pigmentation (or variably pigmented) within the conjunctiva or onto the cornea. A simple biopsy can determine whether a pigmented conjunctival tumor is a benign nevus, primary acquired melanosis, or conjunctival melanoma.
Lymphoma can also occur in the conjunctiva. These tumors look like red or salmon-colored patches on the eye and can be the first sign of systemic lymphoma. Eye cancer specialists usually biopsy lymphoid tumors so that a pathologist can perform special immunologic and genetic studies on the tumor cells. These techniques are used to determine if the tumor is benign or malignant. Patients with lymphoid conjunctival tumors should have a complete medical check up and be examined by a hematologist-oncologist. Other “less common” conjunctival cancers are reviewed in this section.
Symptoms
Most conjunctival tumors do not cause symptoms. Patients typically seek medical attention because they notice a discoloration on the eye or extension of the tumor onto the cornea. Conjunctival tumors can also be found by an eye care specialist during a routine eye examination.
Diagnosis
Most small benign-appearing conjunctival tumors can be photographed and followed for evidence of growth prior to biopsy or treatment. If they are raised, hypervascular or extend onto the cornea a biopsy is more reasonable. At The New York Eye Cancer Center we typically obtain an office-based cytology specimen for squamous carcinoma. This lets us know the tumor is squamous and avoids a trip to the operating room. In contrast, both melanoma and lymphoma require more histopathology and special pathology analysis. Therefore, those tumors require surgical biopsy or if small, excision.
Conjunctival melanomas require special treatment. The natural history of these tumors has been characterized as presenting with multiple tumors or non-pigmented skip areas.
Therefore, it is difficult and some think impossible to define the extent of the tumor on clinical examination.
The So-Called “No Touch Technique”
The natural skip areas of pigmentation, multifocal presentation and high rates of recurrence have led some eye cancer specialists think that handling conjunctival melanoma promotes spread. They fear that tumor cells get stuck on the instruments that if reused, implant tumor on other, unaffected parts of the globe.
However, Dr. Finger disagrees with this theory and its so called “no touch technique” that requires surgeons to get new instruments after each time they touch the tumor (to prevent transplantation). However, there are no other cancers where surgeon-related transplantation has been found. More likely, these eye cancer specialists operate on one area, thinking that the pigmented portion of the tumor is the complete extent of disease. Unaware, there are other non-pigmented or small tumors that are not yet visible and later grow. Then they think they transplanted the tumor.
At The New York Eye Cancer Center, when conjunctival melanoma is suspected, Dr. Finger utilizes his specially designed cryotherapy devices “Finger-tip” cryotherapy probes” to make sure the tumor and a surround of normal appearing tissue is treated before he touches the tumor. Then the tumor can be safely removed without fear of transporting tumor cells or invaginating the edges of the wound rendering tumor too deep to treat with chemotherapy eye drops. At The New York Eye Cancer Center, topical chemotherapy eye drops are used for treatment of both squamous and melanoma cancers. These drops have been found to reduce or more commonly eliminate the need for extensive surgery.
Evaluation of the biopsy specimen should be performed by an experienced ophthalmic pathologist. If there isn’t an ophthalmic pathologist in your area, you can request that the histopathology slides be sent for second opinion.
Treatment: General Guidelines
Small tumors can be completely removed, and if they are found to be either squamous carcinoma or malignant melanoma, additional cryotherapy (freezing) is likely to improve local tumor destruction and thus prevent recurrence. Dr. Finger has developed specialized “Finger-tip” cryotherapy probes to uniformly freeze large surfaces of the eye with minimal intraocular penetration (see innovations section).
Chemotherapy Eye Drops:
Conjunctival melanoma and squamous carcinoma can be difficult to treat if they are “mulitfocal” – occur in multiple spots on the eye. In these cases, even surgical removal with freezing therapy may not control the tumor. Dr. Finger has found that “Chemotherapy eye-drops can be used for and are often better than surgery for most patients with conjunctival cancers.” Chemotherapy eye-drops treat the entire surface of the eye, are less dependent upon defining the tumors edges, and decreases the chance of scarring (symblepharon) after surgery. Researchers at The New York Eye Cancer Center recently published on treatment of “Giant Conjunctival Squamous Carcinoma’ with chemotherapy eye drops alone (no surgery).
Systemic lymphoma can usually be treated with standard chemotherapy that is also likely to cure malignant ocular lymphomas. If the eye is the only site of malignant lymphoma, low dose external beam radiation therapy is commonly employed.
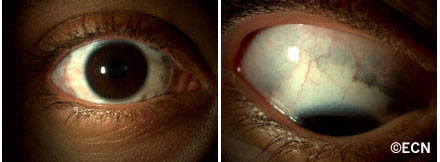
Note the increased pigmentation of the eyelid and episclera. This patient was also noted to have heterochromia (different colored irides) and a darker fundus (more pigment in the choroid) by ophthalmoscopy.
Patients with the Nevus of Ota have increased amounts of melanin (pigment) and melanin producing cells (melanocytes) in and around their eyes. This includes the intraocular blood vessel layer called the uvea (choroid, ciliary body, and iris), on the white part of the eye ball (sclera), and in the eyelids.
Patients with the Nevus of Ota have been shown to be at greater risk for the development of intraocular and central nervous system malignant melanomas (e.g. choroidal melanoma). Though intraocular melanomas are more common in these patients, their lifetime risk is though to be 4%.
Patients with the Nevus of Ota should be examined at least every 6 months by an eye-cancer specialist and a neurologist.
Symptoms
The Nevus of Ota appears as increased pigmentation of one eye and its eyelids. The eyelid is darkened, pigment can be observed on the white of the eye and that iris may be darker (compared to the contralateral iris). Though none of these findings produces physical symptoms, physical asymmetry can have a psychological impact on the patient.
Ocular Melanosis is diagnosed in cases of ocular melanosis there is no eyelid involvement.
Diagnosis
Ocular Melanosis: Episcleral and uveal hyperpigmentation without eyelid skin involvement is called “Ocular Melanosis”
Careful inspection of any patient with two different colored irises (heterochromia irides) may uncover the eyelid and episcleral pigmentation diagnostic of the Nevus of Ota.
Slit-lamp biomicroscopy is used to distinguish between conjunctival and episcleral pigmentation. Comparative examination of the irides can be used to evaluate coloration and surface characteristics.
Dilated ophthalmoscopy similarly demonstrates asymmetric “darker” pigmentation of the choroidal vascular layer beneath one retina.
Ophthalmic ultrasound imaging will reveal thickening of the vascular uveal layer of the eye. Examinations should include both posterior and anterior segment (UBM) imaging.
Treatments
Most patients with the Nevus of Ota have no subsequent related problems.
Less than 4% can develop choroidal melanoma in the affected eye. Fewer will develop intracranial neoplasia. Therefore, it is reasonable for all patients with the Nevus of Ota to have twice yearly eye examinations with dilated ophthalmoscopy. They should also have an initial neurology assessment, followed by periodic medical evaluations.
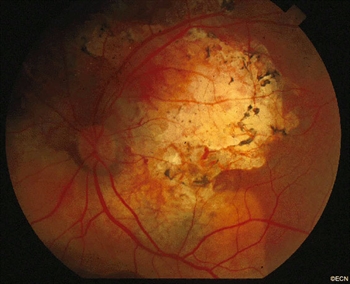
Choroidal Osteoma: Note that the tumor surrounds the optic nerve and it has a relatively light color. There is pigment over the tumor surface and it has scalloped edges. In this case (and at this time) no subretinal neovascularization is present.
Choroidal osteoma are boney tumors that can grow within the eye. They arise within the blood-vessel layer “choroid” beneath the retina. Choroidal osteoma are usually found near the optic nerve and can cause vision loss. The choroidal osteoma impedes the circulation to (and harms) the overlying retina and can be associated with overlying retinal atrophy and adjacent subretinal neovascularization (or, the formation of new blood vessels).
Symptoms
Most choroidal osteomas do not cause any symptoms. They are found on routine eye examination. However, they can be associated with the development of subretinal neovascularization (particularly at the edges of the osteoma). If in the center of the macula, the blood and neovascularization can cause distortion or loss of vision.
Diagnosis
A choroidal osteoma is characterized by bone in the choroidal vascular layer of the eye. These bone deposits are more likely to be found near to the optic nerve, and they are relatively flat (typically less than 2 mm thick). By looking into the eye (i.e., performing an ophthalmoscopy), your doctor will see the yellow tumors, scalloped edges, formed vessels within the tumor, some pigment clumping on its surface, and, rarely, blood associated adjacent subretinal neovascularization.
In the adult or peripheral form of the disease, the doctor might just see the tumor eroding through the overlying retinal pigment epithelium like the tip of an iceberg. In these cases, the extent of the base of the tumor might only be measured by ultrasound imaging.
Photography is used to document the choroidal osteoma size and shape. Baseline photographs are helpful for subsequent evaluations for growth and neovascularization.
A few tests additional tests may be performed in order to confirm diagnosis:
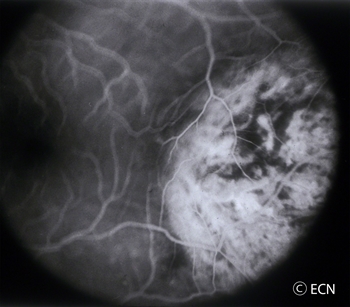
Fluorescein angiography: Since a choroidal osteoma is made of bone, when fluorescein dye circulates through the eye, it will be slow to penetrate the tumor. Once the fluorescein dye is inside the choroidal osteoma, it also has trouble getting out. This is why the fluorescein pattern of choroidal osteoma is one of slow uptake and persistent “late” fluorescence.
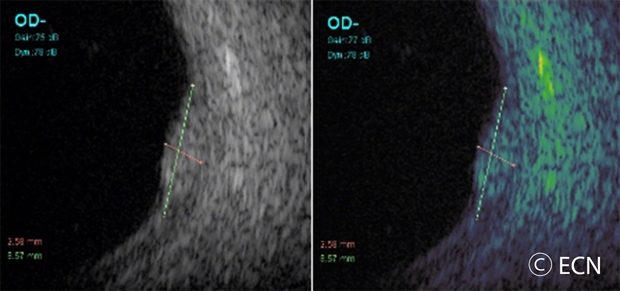
Ultrasound: Ultrasound examination of an eye with a choroidal osteoma will demonstrate intense reflectivity from the hard bony tumor with resultant shadowing of the posterior orbital contents. If the intensity (gain) of the ultrasound machine is decreased, the eye-care specialist is likely to see persistentm characteristic very high reflectivity or “brightness” from the tumor. Ultrasound can also be used to measure the thickness of a choroidal osteoma.
Radiographic imaging: Computed tomography (CT) can be particularly helpful to see the calcification of a choroidal osteoma in unusual cases.
Treatments
Choroidal osteoma is a benign tumor; therefore, most patients do not require treatment. Choroidal osteoma related vision loss is not usually treatable. On occasion, a choroidal osteoma may be associated with subretinal neovascularization (abnormal blood vessels beneath the retina), which are typically treated with laser.When these abnormal vessels are on top of the tumor or near the central vision, intraocular anti-VEGF drugs may be advised.
Eye tumor specialists request that choroidal osteoma is monitored with periodic dilated ophthalmoscopic examinations.
Like a raised freckle on the skin, nevi can also occur inside your eye. The most common “choroidal nevus” or eye nevus are unusual and can only be seen by an eye care specialist. Like a nevus on the skin, a choroidal nevus can grow into a malignant melanoma.
A choroidal nevus rarely requires treatment. Photography is typically used to document the size of the choroidal nevus. If the choroidal nevus has orange pigmentation, if the nevus is leaking fluid, or has a thickness of 2 mm or more it may be (or become) a malignant choroidal melanoma.
Depending on its appearance, patients with a choroidal nevus should have their eyes examined (at least) every 6 months. Only your doctor can look inside your eye to see if the choroidal nevus has changed. If the choroidal nevus has orange pigment or has thickened, it should be checked more often. If a choroidal nevus is leaking subretinal fluid, this is a particularly ominous sign. Such tumors should be followed most closely for evidence of growth or malignant transformation into a choroidal melanoma.
It is reasonable to have an eye cancer specialist check to see if your choroidal nevus looks suspicious and take baseline measurements. This examination may include the use of ultrasound, specialized photography, optical coherence tomography or an intraocular angiogram. It is a good idea for each patient to keep a picture of your choroidal nevus. This picture can be compared to future examinations to help determine if the nevus has changed or stayed the same.
Symptoms
A benign choroidal nevus (eye freckle) rarely causes symptoms. However, if a choroidal nevus leaks fluid or is associated with the growth of abnormal blood vessels (neovascularization) patients can become symptomatic. Such changes can cause a localized retinal detachment/degeneration, flashing lights and loss of vision.
A typical choroidal nevus is asymptomatic or “causes no symptoms” and found by routine dilated eye examination with ophthalmoscopy.
Diagnosis
This image demonstrates how a suspicious choroidal nevus can demonstrate focal leakage on fluorescein angiography.
Choroidal nevus is typically a pigmented tumor of the blood vessel layer (choroid) beneath the retina. A choroidal nevus is typically gray but can be brown, yellow or variably pigmented. Your eye care professional will look to see if the choroidal nevus is raised (has thickness), orange pigment (lipofuscin), or is leaking fluid (retinal detachment). If the choroidal nevus has one or more of these findings, it is labeled a suspicious choroidal nevus that has a chance of turning into or even being a small choroidal melanoma.
A choroidal nevus can have yellow-white spots on its surface called drusen or drusenoid retinal pigment epithelial detachments (DRPED).These are signs of retinal dysfunction. The nevus may be preventing the eye from removing retinal waste products or creating microscopic leaks beneath the retina.There are no studies that show how long it takes for drusen to form on a choroidal nevus.
Treatments
A benign choroidal nevus requires no treatment and there is no way to safely remove them. Since a choroidal nevus can turn into a choroidal melanoma, it is reasonable to have it periodically observed by your eye care professional.
Additional Info
Dr. Finger believes that since skin and conjunctival melanomas have been linked to ultraviolet exposure, and since choroidal melanomas are more commonly found in patients with blue eyes, outdoor occupations, and in Australia (where there is an ozone hole); it is reasonable to wear ultraviolet (UV) blocking sunglasses. Dr. Finger says, “Think of sunglasses as sun block for your eyes.”™
Malignant tumors from other parts of the body can spread into and around the eye. Though they are the most common intraocular cancer in adults, they usually go undetected. This is because most ocular metastases go undetected unless they affect vision, are visible to the patient, or push the eye forward. Eye metastasis are most commonly found in the vascular choroid (choroidal metastasis) within the eye.
Ocular or eye metastasis are usually from a breast cancer (in women) and lung cancer (in men). Other less common sites of origin include the prostate, the kidney, the thyroid, and gastrointestinal tract. Blood cell cancer (lymphoma and leukemia) can also metastasize into the eye and orbit. In 18% of patients, the primary source of the metastasis may be undetectable. In these cases, Dr. Finger may have to biopsy the ocular tumor to obtain tissue for pathology (to determine the primary source).
Symptoms
As stated, most patients with choroidal metastasis have no symptoms. However, if the metastasis is on the eye or eyelids, it may be visible. If the metastasis is located behind the eye (in the orbit), the eyeball may be visibly displaced out or to the side. If the metastasis is within the eye (the most common), metastasis patients can can have symptoms of flashing lights, floating spots or distortion of their vision. In that waiting until patients are symptomatic may be too late to preserve vision, Dr. Finger suggests that all patients with a history of metastatic cancer should have periodic eye examinations.
Diagnosis
In that most patients with ocular metastasis have either a known primary cancer and/or metastatic tumors in other parts of their body; a careful medical history is important. Patients know of prior cancer history and many can remember their tumor stage. History taking can also uncover the signs or symptoms of these other cancers. If an eye cancer specialist suspects ocular metastasis, both eyes and orbits should be examined because ocular metastases can be both bilateral and/or multifocal.
Choroidal metastasis is usually non-pigmented (except metastatic melanomas), and has typical ultrasound and angiographic patterns. Choroidal metastasis is usually poorly circumscribed and can cause retinal detachments. They may have spicules of pigment on their surface. Fluorescein angiography may reveal a typical, “starry sky” of hyper-fluorescent micro-aneurysms. Unlike primary choroidal melanoma, they can grow quickly (weeks) and may require prompt treatment.
The patient with metastasis to the eye should also be examined by a medical oncologist. A complete metastatic survey should be performed to “stage” the patient (to see if there are other tumors within the body). Specifically, radiographic imaging including but not necessarily limited to the brain and lung should be performed due to a high concurrent incidence of intracranial and pulmonary metastases. Dr. Finger will likely suggest a total body PET/CT with fusion.
Treatments
After irradiation, a regressed choroidal metastasis displays spicular hypertrophy of the retinal pigment epithelium.
Most patients with ocular metastasis have either a known primary cancer and/or metastatic tumors in other parts of their body. A careful medical history can uncover the signs or symptoms of these other cancers. If an eye cancer specialist suspects ocular metastasis, both eyes and orbits should be examined because ocular metastases are commonly both bilateral and/or multifocal.a
Choroidal metastasis are usually non-pigmented, yellow or white (except metastatic melanomas). Choroidal metastasis is usually poorly circumscribed and can cause retinal detachments. They may have spicules of pigment on their surface. Unlike primary choroidal melanoma, they can grow quickly (weeks) and may require prompt treatment. They typically have typical ultrasound findings of variable reflectivity, angiographic (starry sky microaneurysm) and OCT wavy surface patterns that are helpful to establish the diagnosis.
Treatment depends on the type of metastasis and its primary source. Treatment options often include chemotherapy, immunotherapy and radiation therapy. In general, chemotherapy and immunotherapy take a relatively long time to work, whereas radiation therapy is more rapid. The choice of chemotherapy, immunotherapy or radiation therapy typically depends on the type of tumor and the temporal “timing” risk for loss of vision.
FAQs
Q: If I have been diagnosed with cancer, and have no symptoms should I get my eye checked? A: It is reasonable to have a yearly-dilated eye examination (with examination of your retina).
Q: If I am on chemotherapy do I need to have radiation too? A: If chemotherapy is controlling your eye tumor you may not need additional radiation therapy.
Q: If I have a metastatic cancer in one eye, can another occur in my other eye? A: Yes, you should be monitored every 3 to 4 months.
Tumors of the eyelids may be benign cysts, inflammations (styes), or malignant tumors (skin cancers). The most common type of eyelid cancer is basal cell carcinoma. Most basal cell carcinomas can be removed with surgery. If left untreated, these tumors can grow around the eye and into the orbit, sinuses and brain. Other eyelid cancers include squamous cell carcinoma, sebaceous cell carcinoma, and malignant melanoma. Together, these tumors make up the remaining 10% of eyelid malignancies.
Symptoms
Most patients with eyelid tumors will notice a nodular growth on their eyelid. This growth can be skin colored, red, brown or black. Malignant tumors may cause loss of eyelashes or distort the position of the eyelid. All patients with eyelid tumors should be evaluated by an eye care specialist with experience in the care of eyelid tumors.
Diagnosis
A simple biopsy can determine if an eyelid tumor is malignant.
Treatments
Malignant tumors are completely removed and the eyelid is repaired using plastic surgery techniques. Some doctors are now using topical immunotherapy or chemotherapy agents to avoid surgery. Dr. Finger can sometime use “Finger-tip” cryotherapy (freezing-therapy) or radiation therapy, depending on the extent of the tumor.
Additional info
A Typical Work-up for a Suspected Malignant Eyelid Tumor:
General: The goal should be total removal of the eyelid cancer. This usually involves primary excision with either frozen section control or the Moh’s technique.
Small tumors are usually removed by pentagonal wedge resection.
Medium-sized tumors often require reconstruction with transpositional flaps (Tenzel, Mustarde, Glabellar).
Large-tumor resections are typically reconstructed with Hughes, Hewes or Cutler-Beard Techniques.
The wall of the eye has 3 main layers. From outside to inside there is: the white sclera, a blood vessel layer called the uvea (choroid, ciliary body and iris) and an inner retinal layer. Further, the pigment producing cells, “melanocytes” are primarily found in the vascular uveal layer. It is those melanocytes that can turn into malignant melanoma. Therefore, when melanoma happens in the choroid, they are called “choroidal melanoma,” the most common primary intraocular malignancy in adults. That said, choroidal melanomas are rare with 5 to10 out of each million people diagnosed with a choroidal melanoma each year. Choroidal melanomas can spread to other parts of the body.
Eye cancer specialists can determine if you have a choroidal melanoma by performing a complete eye examination with testing. This includes asking questions about your medical history, examining both of your eyes, looking into the eye through a dilated pupil, performing an ultrasound examination, and specialized photography (to examine the circulation within the choroidal melanoma).
MOST – Fingers’ Melanoma Mnemonic
Dr. Finger has developed the mnemonic device “MOST” to help eye care specialists to determine if the intraocular tumor is a melanoma.
“M,” Melanoma:
“O,” Orange Pigment Lipofuscin (OPL) a metabolic side product of cell death. This finding tells us that that either the underlying tumor is destroying the overlying tissue or itself is degenerating. Lipofuscin is best seen with a photographic test called Fundus Auto Fluorescence imaging, or FAF.
“S,” Subretinal fluid (SRF) is created by poorly formed or new, “neovascular” blood vessels within the tumor. Cancers need new vessels in order to grow. Large amounts of SRF can be seen by ophthalmoscopy (looking into the eye) and ultrasound imaging. However, small amounts of SRF are best seen on 3D optical coherence tomographic imaging (3D-OCT).
“T,” Thickness of the tumor has been associated with malignancy. Simply, the thicker it is the more likely a pigmented intraocular tumor is malignant. It is widely accepted that tumors greater than 2.0 mm are more likely to be malignant. Ultrasound imaging is currently the best method to measure tumor thickness.
Your specialist will also request that you have a complete general medical check up and specific tests depending upon what they see inside your eye. In the Collaborative Ocular Melanoma Study (COMS), participating eye cancer specialists correctly diagnosed select choroidal melanoma in over 99.6% of cases (without a biopsy). That said, patients with unusual appearing “atypical” tumors were not entered into the study.
Classic Indications for Biopsy
Atypical tumor, metastatic tumor with no observable primary cancer and when the patient requests a pathology diagnosis. More recently, primarily due to genetic testing services, more and more centers are routinely performing choroidal tumor biopsy primarily for genetic tumor analysis. Genetics offers information about the tumor, but does not allow doctors to avoid treatment or follow up systemic testing for metastasis.
Choroidal biopsy has been associated with a risk of hemorrhage, infection, retinal detachment and a poorly quantified risk of tumor seeding (outside the eye). Risks related to tumor seeding are thought to be small, but clearly they have not been evaluated by any large prospective or retrospective study. Each eye cancer specialist should discuss the relative risks (known and unknown) of biopsy prior to surgery.
Questions About Intraocular Biopsy:
Remove the need for surgical tumor treatment?
Reduce the number of radiologic examination or years needed for systemic surveillance?
What are the risks of biopsy (hemorrhage (e.g. vitreous, subretinal, subfoveal), seeding, damage to the lens, optic nerve, retinal detachment, cataract, epiretinal membrane, loss of vision, loss of eye and/or reaction to anesthesia).
Symptoms
Most choroidal melanoma patients have no symptoms. The melanoma is found on routine eye examination. If patients have choroidal melanoma symptoms, they are usually seeing “flashes of light,” noticing “distortion” or loss of vision, and floating objects (floaters) in their vision.
If the choroidal melanoma is in the front of the eye (near the natural lens), it can push or tilt the natural lens causing an irregular astigmatism (blurring of vision).
Choroidal melanoma can leak fluid beneath the retina, making the retina detach and cause symptoms of flashing lights and floating specks “floaters”.
If the choroidal melanoma is in the macula (center of vision), it can grow beneath the fovea making the patient far-sighted. The choroidal melanoma can also grow into and destroy the fovea causing distortion, loss of vision or changes in color perception.
It is important to note that most patients with choroidal melanoma have no symptoms at all. Their tumors are found when they visit their eye doctor for a “routine” eye examination. So everyone should have periodic eye examinations (including dilated ophthalmoscopy). In general, the earlier and smaller the choroidal melanoma, the better the prognosis for both life and sight.
Other, more unusual presentations of anterior choroidal and iridociliary melanoma are discoloration of the iris, a brown spot on the outside of the eye, an irregularly shaped pupil and glaucoma.
Diagnosis
Choroidal melanoma is usually seen by ophthalmoscopy (when your eye doctor looks through a lens into your dilated pupil). Choroidal melanoma has typical “diagnostic” characteristics that include but are not limited to: pigmentation, low to moderate internal ultrasound reflectivity, clumps of orange pigment lipofuscin on its surface, leakage of subretinal fluid, or retinal detachment (on or around the choroidal melanoma) and thickness.
Pigmentation is due to naturally occurring melanin that comes from melanocyte cells in the choroidal layer of the eye. Choroidal melanomas are most commonly pigmented, but can be variably pigmented and even non-pigmented (amelanotic). Non-pigmented choroidal melanoma is due to a proliferation of melanocytes that have lost their ability to make the melanin pigment.
Orange pigment is made up of a chemical called lipofuscin and appears on the surface of choroidal melanomas. Lipofuscin is a product of cell death which indicate that cells are dying on the tumor’s surface. This is also sign of metabolic activity. Melanomas are more metabolically active than choroidal nevi.
Ultrasound is typically used to measure the choroidal melanoma size, evaluate internal tumor reflectivity, and look for melanoma extension behind the eye into the orbit called extrascleral extension. Ultrasound imaging has demonstrated that most choroidal melanomas are shaped like a dome and less commonly like a mushroom. Ultrasound can also evaluate and detect choroidal melanoma associated retinal detachment. However, optical coherence tomography (OCT) is a more sensitive way to detect subretinal fluid – retinal detachment.
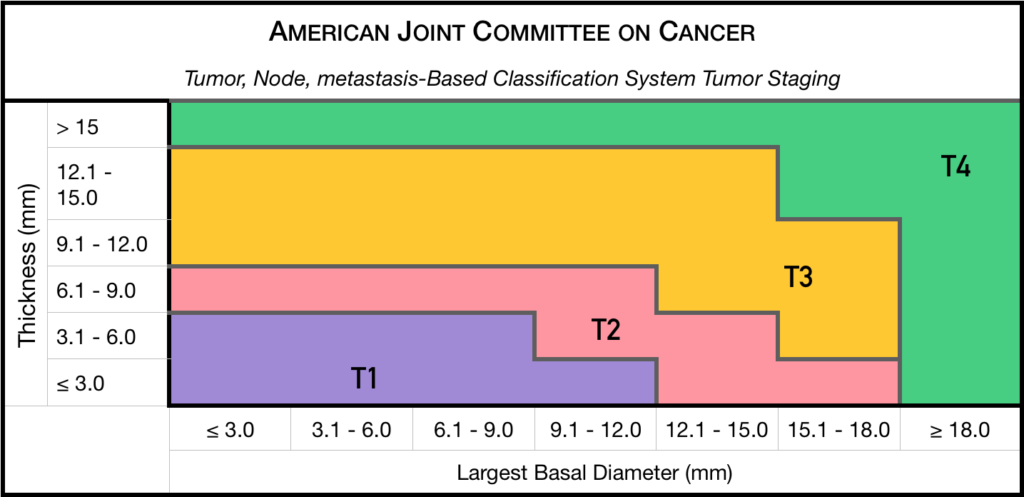
Staging
Chaired by Dr. Paul T. Finger, a committee of top ophthalmic specialists assembled to form the AJCC-UICC Ophthalmic Oncology Task Force. To ensure a broad range of specialists, Dr. Finger “internationalized” the committee, including over 58 members both from the USA and around the world.
This committee had one driving goal: to design a clinically useful Tumor-Node-Metastasis (TNM) based classification “language” for ocular tumors. This first-of-its-kind classification system has become a universal language for all who diagnose and treat ocular tumors.
Not only does a universal classification system offer cancer staging for the patient, it also allows physicians to directly compare data. In the long run, a common “eye tumor” language helps usdetermine and differentiate treatment types as well as coordinate the efforts of researchers working for a cure.
Dr. Finger has since translated this staging system for the worlds’ Union International for Cancer Control (UICC), and offered it to the world. In order to get everyone to employ this new language, he has recruited all the major medical journals to require eye cancer researchers to use AJCC-UICC staging.
Treatments
Small Choroidal Melanoma (AJCC T1 and T2): Patients with a small choroidal melanoma can be treated after their first visit, but since growth helps to prove that the tumor is a cancer, your doctor may suggest “observation” or watching for a small amount of choroidal melanoma growth prior to treatment. Your eye cancer specialist should discuss the relative risks and potential benefits of “observation for growth” as compared to “immediate treatment” for choroidal melanoma. If growth is documented (typically within 6 months of observation), eye cancer specialists will typically recommend definitive treatment.
Medium-sized Choroidal Melanoma (AJCC T3 and T4): Most patients with large-sized choroidal melanoma can be also be treated with eye-sparing low energy radiation therapy (e.g. palladium-103). However, larger tumors require more radiation and larger irradiated intraocular volumes resulting in greater risk of radiation side-effects and poor vision. Rarely such eyes have to be secondarily removed. Eye cancer specialists try to preserve eyes, even if the eye had reduced vision.
Large-sized Choroidal Melanoma: Very large choroidal melanomas (greater than 22 mm width) may be treated by initial removal of the eye (enucleation). This is because the amount of radiation required to destroy a choroidal melanoma that fills most of the eye will likely be too much for the eye to tolerate.
However, most patients, even with very large-sized choroidal melanoma can be treated with eye-sparing radiation therapy. However, after eye sparing radiation for very large choroidal melanomas, eyes are at greater risk to have poor vision, secondary inflammation and may require secondary removal at a later date.
Additional Info
Patients often ask why they have a choroidal melanoma. While there is no one cause, choroidal melanoma is more common among patients with blue vs. brown eyes, those with outdoor occupations, and in Australia where there is a hole in the ozone layer. Therefore, though this hypothesis has yet to be proven, it seems reasonable to assume that choroidal melanoma is related to sunlight (ultraviolet exposure).
In that sunlight exposure has been linked to several eye cancers and diseases of the eye, Dr. Finger suggests that you “Think of Sunglasses as Sun Block for your Eyes” ™ and start wearing your UV blocking sunglasses. They make great gifts too!
Dr. Finger also often gets questions related to stage and spread. These two things are closely linked––choroidal melanoma size is most closely related to its risk for spread to other parts of the body (metastasis). In three separate studies, cumulatively involving almost 20,000 patients, the average rate of metastasis has been 50%. However, patients with smaller tumors have much lower rates compared to larger tumors. Therefore, patients should ask their eye cancer specialist about their tumors AJCC-UICC tumor size and risk for metastasis. In general, the larger the choroidal melanoma the worse the prognosis for both vision and metastasis.
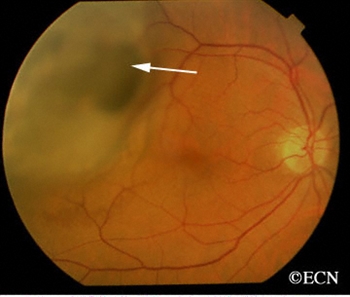
Hemangiomas can grow within the blood vessel layer beneath the retina called the choroid. If they are located in the macula (center of vision) or they leak fluid (which causes a retinal detachment or cystic changes in the retina), they can affect visual acuity. However, many choroidal hemangiomas never grow or leak fluid and can be observed without treatment. Choroidal hemangiomas are not cancers and never metastasize.
Symptoms
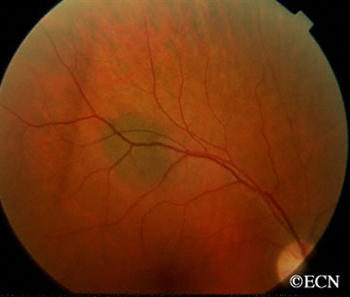
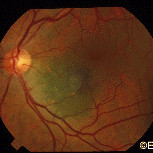
<justify?This choroidal hemangioma lies above the optic nerve, but extends into the fovea. Though there was no serous detachment, cystoid retinal degeneration of the fovea caused decreased visual acuity to 20/200.
On your left, there is a red colored choroidal hemangioma just above the round optic nerve. Typically, choroidal hemangioma are reddish to orange colored. They can have areas of increased pigmentation which can make them difficult to differentiate from choroidal melanomas.
By lifting the overlying retina, choroidal hemangiomas can cause far-sightedness (hyperopia), distorted vision (metamorphopsia), flashing lights, or blurred vision. Choroidal hemangioma that cause no symptoms at all, are usually found on routine dilated eye examinations (ophthalmoscopy).
Diagnosis
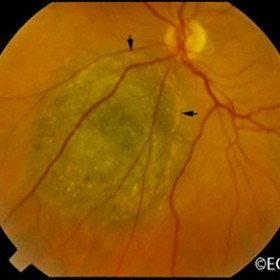
Course Vascular Pattern
Intraocular Photography and Angiography: An eye care specialist can perform studies of the blood flow within the eye by injecting drugs called fluorescein or indocyanine green. They can also look at the overlying blood vessels with computerized optical coherence tomography – angiograpy (OCT-A). When drugs are injected into the arm or hand, they will travel into the blood vessels inside the eye. Using special lights that make the angiographic dyes fluoresce, your doctor can see special differentiating circulation patterns, that help differentiate between the types of tumors. For example,choroidal hemangioma have a unique pattern of circulation where the large blood vessels produce a “COARSE VASCULAR PATTERN.”
Ultrasound Imaging: Sound waves can also be used to examine the inside of the eye. Ultrasound images of a choroidal hemangioma reveals that they are “bright.”This is because they are a mass of relatively large and well-formed blood vessels. Each blood vessel reflects sound waves producing characteristically intense reflections or moderately “MODERATELY HIGH INTERNAL REFLECTIVITY” from within the hemangioma tumor. Moderately high internal reflectivity is an important diagnostic characteristic.
Choroidal Hemangioma high internal reflectivity
Treatments
When a choroidal hemangioma is not causing symptoms, leaking or damaging the eye; it can be photographed and followed for evidence of change prior to treatment. However, if the choroidal hemangioma is documented to grow into the center of vision or is causing a retinal detachment or angle-closure glaucoma it is treated to save vision.
Hot Laser: Laser photocoagulation had been used to decrease the amount of fluid leaking out of choroidal hemangioma. Unfortunately, laser results are usually temporary and recurrence of retinal detachment or cystoid retinal degeneration usually results vision loss.
Photodynamic Therapy (PDT) is a cold or non-thermal laser treatment that involves injecting a light-sensitive dye into the patient and then shining a dye-activating PDT laser light on the choroidal hemangioma. The light-activated dye causes the abnormal blood vessels to close, shrink, and stop leaking. However, PDT requires that the tumor can be visualized during treatment. So, PDT will not work if there is a large retinal detachment covering the tumor or if the tumor is located too far anterior inside the eye. When it works, PDT offers a more long-term method to treat leaking posterior choroidal hemangiomas. The dye is expensive and multiple treatments are usually required. Lastly, due to changes in treatment patterns for AMD, fewer and fewer PDT laser machines and experienced PDT-laser surgeons exist.
Radiation Therapy: At The New York Eye Cancer Center most patients are treated with low-dose external beam or implant radiation therapy. Radiation has been used used to treat leaking choroidal hemangiomas for decades. The differences are, that in the past relatively large doses of radiation were used and some collateral radiation damage occurred. However, modern radiation techniques involve much lower doses of radiation as well as implant techniques that better focus the treatment area. Low dose radiation typically requires a total of less than two weeks of daily treatments. In Dr. Fingers’ experience, almost all choroidal hemangiomas and their associated retinal detachments can be cured with low dose radiation therapy.
Summary
Choroidal Hemangioma are benign tumors made up of blood vessels. Since choroidal hemangioma do not metastasize (spread to other parts of the body), we are more concerned with damage they can cause within the eye. Choroidal hemangioma can be stable and not require treatment. Others can change a patient’s vision by displacing the retina causing hyperopia (far-sightedness), causing degeneration of the overlying retina (cystoid degeneration), or by leaking fluid under and detaching the retina (serous retinal detachment).
Most choroidal hemangioma are treated if they induce a retinal detachment. Also in rare cases, choroidal hemangioma can fill most of the eye, affect the iris or be associated with the Sturge-Weber Syndrome. In these cases, the choroidal hemangioma (due to its increasing thickness) can cause angle closure glaucoma. In these cases, radiation can be used to cause regression and thinning of the hemangioma in the iris and prevent vision loss.
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.