The benign eyelid tumor hydrocystoma comes from the Latin hydro, meaning fluid, and cystoma, meaning cyst or sac.
A hydrocystic thickening is an epithelial-lined serous cyst (within the skin or soft tissues). Sometimes it looks like they are translucent.
Symptoms
An intradermal epithelial-lined serous cyst.
Hydrocystomas most commonly occur on the eyelids. They typically are the same color as eyelid skin, rounded and soft to the touch. They are slow growing, may cause misdirection but not loss of eyelashes.
Diagnosis
Hydrocystoma is a benign tumor that can be photographed and followed for evidence of growth. High-frequency ultrasound can demonstrate that the tumor is filled with fluid and confirm the diagnosis.
Treatments
Excision is typically performed if growth is documented, basal cell or other eyelid cancer is suspected and for cosmetic reasons. During removal, your surgeon will try and keep the cyst intact. Removing the whole tumor will help keep it from recurring.
These tumors typically grow and then spontaneously decrease in size.
Congenital “strawberry-spot” which usually will spontaneously get smaller “involute.”
Treatment is indicated for the prevention of amblyopia (loss of vision) and strabismus (misdirected eyes). These tumors naturally grow and then spontaneously decrease in size. Therefore, if the tumor is not harming the child, it can be observed untreated for spontaneous regression.
Symptoms
Capillary hemangiomas are typically found at birth. They will grow during the first decade (10 years) and most will shrink (involute). If they involve the eyelids, they can cover the eye and cause loss of vision (amblyopia). It is very important that children with capillary hemangiomas be seen by a pediatric ophthalmologist and eye cancer specialist immediately.
Diagnosis
Capillary hemangioma is diagnosed by clinical examination. It has a typical appearance and biopsy is rarely needed. It appears as a reddish tumor or mass beneath the skin. The eye care specialist will order a radiographic scan (MRI or CT) to see how deep the tumor extends into the orbit (around the eye). The child’s pediatrician should be advised and the child inspected for hemangiomas on other parts of the body.
Treatments
Observation for spontaneous resolution is commonly performed. If the tumor is blocking the eye and vision causing amblyopia, then it can be treated with an oral beta-blocker medication (e.g. propranolol) or injected with a steroid solution. This will shrink the tumor in an effort to uncover the eye. Surgery may be required to remove very large tumors. The child’s pediatric ophthalmologist may suggest that the other “good” eye be periodically covered with a patch to strengthen the tumor affected eye and prevent amblyopia-related vision loss.
A basal cell carcinoma anterior to the medial canthus: Note the pearly margins and the central crater.
The most common type of eyelid cancer is basal cell carcinoma. Most basal cell carcinomas can be removed with surgery. However, many older patients will try to ignore these slow growing tumors. However, it is important to know that when leftuntreated, these tumors can grow around the eye and into the orbit, sinuses and brain. Basal cell carcinomas are more commonly found on the lower eyelids and almost never spread to other parts of the body (metastasize).
Symptoms
Patients with basal cell carcinomas most commonly notice a reddish nodule slowly forming on their eyelid. The tumor is most commonly found on the lower eyelid, followed by the medial canthus (skin toward the nose) and can occur on the upper eyelid. Eyelash loss (around the tumor) suggests that a basal cell carcinoma is malignant.
Less commonly, basal cell cancers can be pigmented or present without any nodule at all. When the tumor does not make a nodule and grows within the eyelid, it can induce pulling of the eyelid (away from the eye). Doctors call this form of basal cell carcinoma “morpheaform,” which are much more difficult to cure because its edges are harder to define.
Diagnosis
Though small tumors can be photographed and followed for evidence of growth (prior to biopsy); once your eye cancer specialist suspects basal cell carcinoma, most eye cancer specialists will suggest tumor biopsy. This specimen is sent to the pathologist to confirm the diagnosis prior to complete removal or treatment of the tumor. Biopsies can be performed in the doctor’s office, or in the operating room prior to definitive treatment.
Treatments
Once the diagnosis is confirmed by the pathologist, treatment will be recommended. Wedge resection and Moh’s surgery require the surgeon continue to remove the tumor until the margins (edges) are negative (free of tumor). Unlike most skin, the eyelid are a complex functional apparatus that requires special reconstruction techniques.
Most basal cell carcinomas are cured when they are small. Unfortunately, some patients choose to ignore or deny the existence of these tumors. Those patients allow their tumor to invade behind the eye and become difficult or impossible to remove. In these cases, combinations of surgery, radiation and chemotherapy may be required to control or destroy the tumor.
Additional Info
This is a sun related cancer. Dr. Finger suggests, “Think of sunglasses as sunblock for your eyes”™
Squamous conjunctival neoplasia (SCN) is most commonly found in older white males (76%). The average age of patients affected by SCN is 56. This tumor, said to make up 14% of all primary ocular and orbital tumors is related to sun exposure. Sunlight, particularly ultraviolet-B (UV-B) radiation can cause DNA damage, mutations, and cancerous cells. Though human papillomavirus -16 has been found in conjunctival tumor specimens, it has not been proven to cause this tumor. The immunosuppressed (e.g. elderly, HIV positive) are particularly vulnerable. When conjunctival squamous carcinoma occurs in HIV positive patients, it can be particularly resistant to treatment.
Symptoms
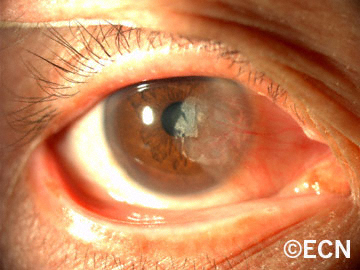
Patients notice a white or yellow-white tumor on the surface of the eye (often with extension onto the cornea).
Diagnosis
Squamous conjunctival neoplasia tends to be found between the eyelids (interpalpebral space), and at the limbus (border of the white sclera and clear cornea). This tumor can extend onto the cornea, around the limbus, and rarely into the eye and orbit. When the tumor extends onto the cornea it can be avascular and opaque in appearance. Commonly, squamous conjunctival neoplasia will contain characteristic corkscrew-shaped blood vessels.
Squamous Conjunctival Carcinoma: Note the white nodular thickening at the limbus.
Nodular Squamous Conjunctival Carcinoma: There is also a nodular type that is circumscribed, rapidly growing, and invasive. Since this type more commonly extends beneath the conjunctival epithelium, nodular tumors exhibit increased metastatic potential. All large squamous conjunctival cancers should be examined with high frequency ultrasound. This technique can be used to determine if the tumor has invaded the eye or orbit.
In the image on the middle right, note that a few corkscrew-shaped blood vessels on its surface (arrow).
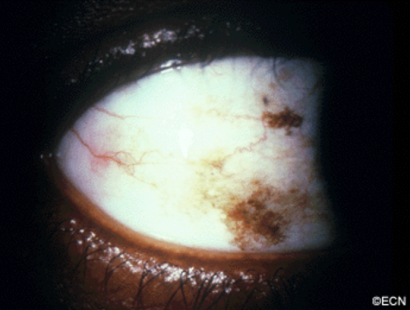
Diffuse Squamous Conjunctival Carcinoma:
Nodular Squamous Conjunctival Carcinoma: Note that a few corkscrew-shaped blood vessels on its surface (arrow).
There is a diffuse variant that can masquerade as chronic conjunctivitis. Tumor thickening occurs late making it difficult to diagnose. Therefore, a conjunctival biopsy should be considered in cases of conjunctivitis lasting more than 3 months.
The diagnosis of malignant squamous conjunctival neoplasia is typically made by biopsy. Like most squamous epithelial tumors, invasion beneath the epithelium into the substantia propria defines these lesions as carcinoma. This is because, when the tumor is contained within the epithelium it does not have access to the lymphatic system or metastatic potential.
Treatments
Every suspected squamous conjunctival cancer should be photographed and AJCC staged prior to biopsy or excision. Surgical excision (alone) has been associated with high rates
The diagnosis of squamous conjunctival neoplasia is typically made by biopsy.
of recurrence. This is because the tumor’s edges and deep margins are either gray or the same color and the sclera and thus difficult to determine. When the tumors edges are clear and avascular, it leads to a false sense that the tumor is smaller than it is.
Local superficial freezing of the tumor bed, sclera and adjacent conjunctiva (cryotherapy) has improved local control and decreased the incidence of tumor recurrence. Other centers have added radiation therapy to decrease tumor recurrence.
However, topical chemotherapy is becoming the most common method of treatment.
While a large clinical trial is needed to compare the effectiveness of topical chemotherapy to excision and cryotherapy, Dr. Finger now uses topical chemotherapy eye drops to avoid surgery (in most cases).
Additional info
Local Spread:
Intraocular spread of squamous conjunctival neoplasia is rare in developed countries (< 5% of cases). When intraocular penetration occurs it is typically through the limbus. Signs include neovascularization of the iris and cornea as well as glaucoma, and peripheral anterior synechiae. Dr. Finger has found high frequency ultrasound to be particularly helpful in these cases.
High frequency ultrasound is particularly helpful in these cases. Positive findings include: thickening of the ciliary body, uvea and blunting of the iridocorneal angle. Intraocular penetration is typically treated by deep cryotherapy, eye-wall resection or radiation.
If the orbit is invaded, there is a risk of spread into the sinuses and brain. Such invasion is said to be the most common cause of death related to this tumor. When squamous conjunctival neoplasia metastasizes beyond the eye and orbit, it can either be found in the regional lymph nodes (preauricular, submandibular, and cervical), or in the lungs and bone.
In general, early detection allows for removal or destruction of these tumors with excellent local cure rates.
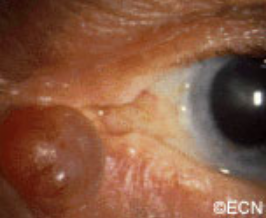
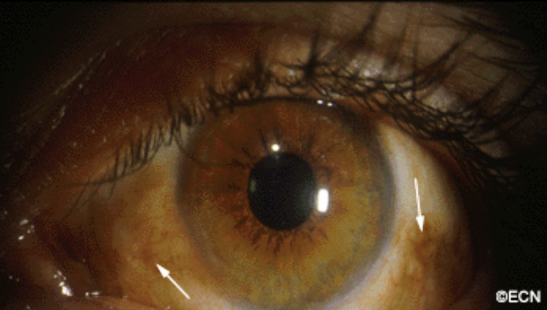
A nasal pterygium is noted to extend onto the cornea.
Pterygium is a vascular pink tissue that can grow from the conjunctiva onto the cornea. If it grows into the line of vision (over the pupillary aperture), it can interfere with vision. Pterygium are most commonly found to originate from on the inner (nasal) surface of the eye, and extend toward the the pupil. They can also occur the on the temporal (towards the ear) side of the eye.
Pterygium are more common in countries near to the equator, where there is long-term exposure to sunlight, particularly ultraviolet (UV) rays. In addition, others believe that chronic eye irritation may play an important role. Therefore, pterygium occur more often in people who spend time outdoors, particularly in sunny climates.
Pterygium are benign (not malignant) tumors. Hence pterygium do not invade the eye, sinuses or brain. Pterygium do not spread to other parts of the body (metastasize).
Symptoms
Pterygium are external to the eye, visibly apparent, and typically noted to grow before they cause symptoms. They can become irritated, causing an itchy, burning sensation. If allowed to grow into the line of vision (pupillary axis), then a pterygium can cause impairment of vision.
Diagnosis
Pterygium is usually diagnosed based on appearance. They are typically a wing-shaped, soft tissue growth from the nasal or less commonly the temporal bulbar conjunctiva toward the cornea. Should growth be documented, excision is usually suggested. When surgery is performed, the excised tissue should be sent to pathology for a histopathologic diagnosis.
Treatments
This pterygium has progressed over the visual (pupillary) axis and is affecting the patient’s vision.
If a pterygium becomes red and irritated, lubricating eye drops or ointments can be placed onto the eye as to reduce the inflammation. Rarely, anti-inflammatory eye drops may be prescribed.
Pterygium are surgically removed when they affect sight, grow such that your eye care professional expects it to impair vision, or if it is cosmetically unacceptable. Unfortunately, pterygium may return despite proper surgical removal. To help prevent recurrences surface radiation, conjunctival implants (grafts), or chemotherapy medications can be used.
Patients with pterygium should wear ultraviolet (UV) protective sunglasses, use artificial tears, and avoid dry and dusty conditions.
A pingueculum is a yellowish patch on the white (sclera) of the eye. Found between the eyelids, it is most often on the nasal side (closest to the nose), but can be found on the temporal (closest to the ear) side. Pingueculum are not cancer. It is a sun-related alteration of the normal conjunctival tissue.
Pingueculum.Pingueculum with thickness: Note the lack of intrinsic vascularity or corneal extension.
Symptoms
Pingueculum are usually visible, found on the surface of the eyeball, between the eyelids. They can become a cosmetic problem, rarely become inflammed, irritated and red. When this happens, the patient may have a feeling like there is something (a foreign body) on the eye.
Pingueculum can become thickened. But, it should not have prominent or corkscrew-shaped blood vessels (within the tumor), nor should the pingueculum extend onto the cornea.
Diagnosis
An eye care professional can diagnose a pingueculum by clinical “slit-lamp” examination.
Treatments
Eye care professionals typically leave pinguecula alone. If it becomes irritated, it can be treated with a topical non-steroidal or steroid eye drop. Artificial tears are also helpful. Surgery is reserved for atypical pingueculum or when another “cancerous” diagnosis is suspected.
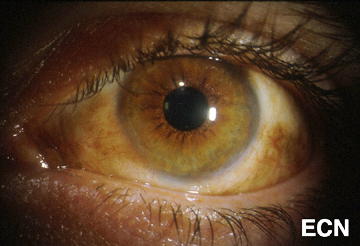
Malignant melanomas can start as a nevus/freckle or arise as newly formed conjunctival pigmentation called primary acquired melanosis (PAM).
A simple biopsy can determine whether a pigmented conjunctival tumor is a nevus, primary acquired melanosis, or conjunctival melanoma. As seen below, primary acquired melanosis typically affects one eye, in middle-aged, fair-skinned people.
In contrast, darkly pigmented individuals often have naturally occurring pigment on their conjunctiva. When this occurs it is called racial melanosis. Unlike primary acquired melanosis, racial melanosis tends to involve both eyes and is typically present for the entire life of the patient.A simple biopsy can determine whether a pigmented conjunctival tumor is a nevus, primary acquired melanosis, or conjunctival melanoma. As seen above, primary acquired melanosis typically affects one eye, in middle-aged, fair-skinned people.
Symptoms
Pigmentation of the surface of the eye and/or eyelids.
Diagnosis
Most pigmented spots on the eye are benign. Your eye care specialist can take a photograph of them and watch to see if they change prior to consideration of biopsy or treatment.
Pigmented conjunctival tumors that are raised, hypervascular, or extend onto the cornea are considered suspicious. Though suspicious conjunctival tumors can be biopsied after your first visit to the eye cancer specialist, close observation for evidence of growth (prior to biopsy) may also be recommended. Documented tumor growth is a strong indicator that biopsy should be performed.
Once the biopsy is performed, the specimen should be evaluated by an ophthalmic pathologist. If there is no ophthalmic pathologist at your center, the slides can be sent for second opinion.
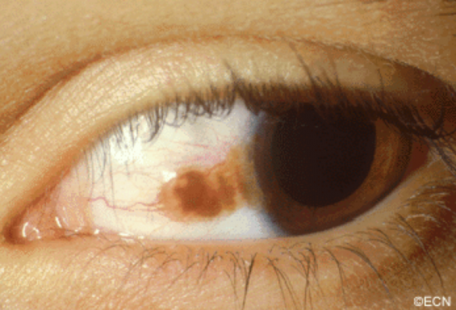
A pigmented conjunctival nevus can be photographed and followed for evidence of growth prior to biopsy or excision. It is important to note that both benign and malignant tumors can grow (though malignant tumors will grow faster).
Slit-lamp photography of benign conjunctival lesions is helpful in determining if subsequent change has occurred. It is a good idea for the patient to have a copy of the initial photograph because doctors are not required to keep medical records indefinitely, and the lesion can change even years after the initial diagnosis.
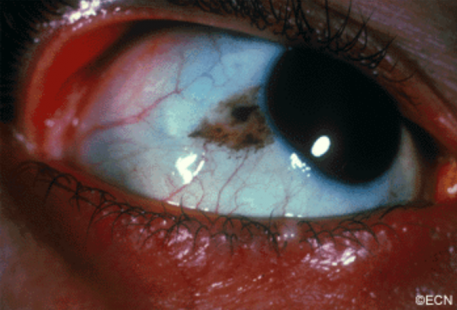
Primary acquired melanosis with atypia (biopsy proven).
Malignant melanoma can occur on the surface of the eye (conjunctiva and cornea). It can start on its own, as a pre-existing nevus or arise within newly formed pigmentation.
Symptoms
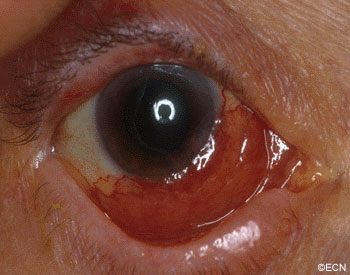
Most patients notice either a nodule forming on, or a darkening of the surface of the eye. Large tumors can bleed resulting in “bloody tears.” The tumor can extend onto the eyelid skin and lymph nodes in front of the ear (preauricular) or neck (cervical). Involved lymph nodes enlarge and can be felt (palpable) during examination.
Diagnosis
The doctor will examine your eyes. This includes an examination of all the conjunctival surfaces (including the inside of the eyelids). Pigmented conjunctival tumors are considered suspicious if they have large blood vessels running toward them, if they extend onto the cornea or if they extend into the conjunctival fornices.
Photographs should be taken of all the conjunctival and corneal surfaces at the time of initial examination (prior to any biopsy). This is important because it helps the doctor document the extent of the condition (stage the tumor) and can be used to plan for surgery and aid in follow up. Removing a conjunctival melanoma prior photography and/or referral to an eye cancer specialist can decrease the patients chance for cure.
Biopsy can determine whether a pigmented conjunctival tumor is a nevus, primary acquired melanosis, or conjunctival melanoma. A conjunctival nevus and benign acquired melanosis can be photographed and followed for evidence of change prior to intervention. Malignant conjunctival melanoma and intra-epithelial melanoma (in situ) should be removed or destroyed.
*Note* In a multicenter international effort to develop a staging system for conjunctival melanoma, the authors agreed that the term Primary acquired melanosis with atypia should be abandoned in favor of conjunctival melanoma in situ.
Treatments
Most very small areas of conjunctival hyperpigmentation can be photographed and followed for evidence of growth or change prior to treatment. If they are raised, hypervascular or extend onto the cornea a biopsy is reasonable. Small tumors can be completely removed, and if they are found to be malignant additional cryotherapy (freezing) or adjuvant topical chemotherapy may be necessary.
Melanomas can be difficult to treat if they occur at multiple spots on the eye. In these cases, surgical removal with freezing therapy may not control this tumor. Then chemotherapy eye-drops can be used for patients with conjunctival melanoma. Chemotherapy eye drops treat the entire surface of the eye, and is less dependent upon defining the tumors edges.
Lymphoma can occur in the conjunctiva. These tumors typically look like “salmon-patches.” Red colored tumors on the eye can be a presenting sign of systemic lymphoma. Eye cancer specialists usually biopsy lymphoid tumors and the pathologist is requested to perform special immunologic and genetic studies on the tumor cells. These techniques are used to determine if the tumor is benign or malignant as well as define the subtype of lymphoid malignancy.
Symptoms
The “Salmon-Patch” of Conjunctival Lymphoma.
Most patients notice the reddish discoloration of the surface of the eyeball (conjunctiva). As the tumor enlarges, patients seek medical attention. Conjunctival lymphomas can become large enough to displace the eyeball, and restrict eye movement. Eye movement restriction can cause diplopia (double-vision).
If the tumor extends behind the eyeball, it can be pushed forward (proptosis). Rarely, and if large enough, orbital lymphoma can press on the optic nerve and cause loss of vision. If discovered early, prompt treatment offers the best chance for recovery of vision.
Diagnosis
Pathology analysis of biopsied tissue allows your eye cancer specialist to determine if thelymphoma is a less aggressive MALT (mucosa associated lymphoid tissue) or the more malignant-behaving non-MALT lymphomas. Clinical differentiation between these types of cancers can be difficult.
In either case, patients with lymphoid conjunctival tumors (ocular adnexal lymphoma) should have a complete medical check up and be followed by both their eye cancer specialist and a hematologist-oncologist.
Treatments
Treatment depends on whether or not systemic lymphoma is detected. If the patient is found to have systemic lymphoma, they are likely to receive systemic immunotherapy or chemotherapy, no additional eye treatment may be necessary. However, if the conjunctival tumor is the only site of disease, most patients with malignant conjunctival lymphoma at The New York Eye Cancer Center are treated with low dose external beam radiation therapy.
This epibulbar dermolipoma is found to infiltrate the peripheral cornea and extend back to the lacrimal gland.
Epibulbar dermoids are benign tumors. They tend to be firm, white-yellow or pinkish tumors straddling the limbus in the temporal (primarily inferotemporal) quadrants. They are located both over the cornea and sclera. They can range from several millimeters to over a centimeter in size. They are typically unilateral (found on one eye), but can be bilateral.
Dermoids are choristomas (normal tissues that are in the wrong place). Made up of cutaneous and subcutaneous tissue, it is not uncommon for dermoids to contain hair and other skin structures. These tumors can be found on the eye, adnexa and orbit.
Dermolipomas are more commonly found in the superotemporal quadrant extending to the lacrimal gland and/or orbit.
Symptoms
Most patients with epibulbar dermoid or dermolipomas have no symptoms unless hairs or other dermal structures cause local irritation. The lesions do cause a cosmetic defect.
Diagnosis
The diagnosis of dermoid and dermolipoma is made by ophthalmic examination. These lesions are typically present at birth and do not progress. Though ultrasound and radiographic imaging may be required to investigate the extent of the tumor, biopsy is not necessary.
Dermoids or dermolipomas are more likely to be associated with Goldenhar’s Syndrome if they are multiple or bilateral. Goldenhar Syndrome is associated with dermoid tumors at the tragus of the ear and facial dysostosis.
Treatments
It is very important to make sure your child does not have a secondary astigmatism related to corneal tumor involvement. Early treatment of astigmatism can prevent amblyopia (loss of vision).
Surgery can be performed to limit the cosmetic defect, but there are many reports of secondary complications related to thinning of the scleral “eye wall” and corneal astigmatism.
Surgical removal of dermolipomas (that can extend into the lacrimal gland and orbit) can be associated with lacrimal gland dysfunction (dry eye) and double vision. Care must be taken to preserve the overlying conjunctiva and lacrimal gland.
Additional Info
Dermoids and dermolipomas can be associated with Goldenhar Syndrome or Linear Nevus Sebaceous Syndrome.
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.