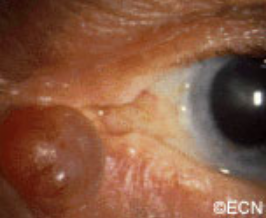
Note the relatively flat surface, red (indurated – inflammed edges, and the white flakey material on the right side of its surface.
Description
Squamous carcinomas of the eyelid can locally invade the orbit and sinuses, but rarely metastasizes. It is the second most common malignant eyelid tumor, but is 10 times less common than basal cell carcinoma. This should not be confused with conjunctival squamous carcinoma, which is the most common conjunctival cancer and can spill over onto the eyelid skin.
Symptoms
Squamous eyelid carcinoma can have symptoms that range from the appearance of a hypervascular flat pale, reddish or flaky lesion on the eyelid skin to a thickened well-demarcated reddish, flat tumor surrounded by inflammation (with or without scaling from its surface).
Diagnosis
Squamous carcinoma of the eyelid should be photographed at baseline. These lesions can remain unchanged (for years), then invade into the dermis and grow. A simple wedge biopsy can be performed and sent for pathologic evaluation. Once the diagnosis of squamous carcinoma is biopsy proven, definitive treatment is needed.
Treatments
Like basal cell carcinomas, squamous cell cancers of the eyelid rarely metastasize. However, they can grow around the eye into the orbit, sinuses and brain. Therefore, early intervention with complete excision or destruction is warranted.
Surgical approaches depend on the doctors training. Eye care specialists will either perform a planned excision with frozen-section control (of the margins) or the Moh’s Technique. Both types of surgery are used to remove the entire tumor along with a safety zone of normal appearing tissue from the edges of surgical wound (margins). No comparative studies have definitively shown that one technique better than the other. Both surgeries require a cosmetic surgical repair to return eyelid function and cosmesis. When the orbit and sinuses are not involved, local excision is usually curative.
Extension into the orbit and sinuses typically requires more extensive surgery (exenteration, sinusectomy) with subsequent radiation therapy.
At the New York Eye Cancer Center, we have treated select patients with small squamous carcinomas of the eyelid with topical chemotherapy agents or freezing (cryotherapy) using “Finger-tip” applicators. Dr. Finger tries to avoid surgery when possible.
Sebaceous carcinoma arises from the glands within the eyelids, caruncle or eyebrow. They are more commonly found on the upper eyelid and in middle-aged patients.
Symptoms
Sebaceous cell carcinoma is suspected due to evidence of eyelash loss and the formation of a yellow-nodule. This tumor can also present as a persistent (months) non-responsive blepharitis or conjunctivitis. In these cases, a high index of suspicion for sebaceous cell carcinoma will lead to biopsy and the diagnosis. Once sebaceous carcinoma is suspected a biopsy is warranted. Before surgery, the pathologist should be advised of this possible diagnosis so the specimen can be processed appropriately
Sebaceous carcinomas are one of the rarest eye cancers and can look like a chalazion (stye) or conjunctivits. In that sebaceous carcinoma can mimick these relatively benign dieases, eye care specialists should be suspicious of this tumor in any patient with persistent conjunctivitis, blepharoconjunctivitis or chronic/recurrent chalazion. Therefore, any conjunctivitis or chalazion that is not getting better after 3 months of observation, should be biopsied.
Diagnosis
Sebaceous carcinoma of the eyelid typically presents as a yellow-nodule in the upper lid. The patient may have history of colon, breast, genitourinary or other skin malignancies (Muir-Torre Syndrome).* When a nodular tumor, it can cause eyelash loss, but is not painful (compared to styes). This tumor can also present as a hypervascular conjunctival tumor and tends to spread along the conjunctival surface. In these cases sebaceous carcinoma looks like conjunctivitis.
It is worth repeating that “any conjunctivitis or chalazion that is not getting better after 3 months of observation should be biopsied.” If cytopathology is available at your medical center, a scrape biopsy of the conjunctiva can be initially performed in the office setting. However, the gold standard for diagnosis of sebaceous carcinoma is histopathologic evaluation of a fresh tissue specimen.
Once the diagnosis is made, a metastatic survey is warranted. Sebaceous carcinoma can spread to regional lymph nodes (pre-auricular and cervical) as well as to lungs, brain, liver and bone. At The New York Eye Cancer Center, we obtain a total body PET/CT scan (from head to toes) for staging. Published series have reported that the occurrence of metastatic disease was dependent on the size and location of the primary tumor and occurred in up to 27% of patients. Local tumor invasion of the lymph nodes, orbit or metastatic sites were associated with a poor prognosis for survival.
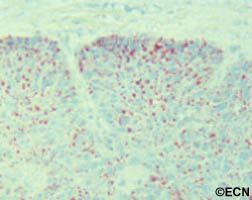
Treatments
Biopsy usually requires a full thickness lid section sent for histopathologic evaluation prior to formalin fixation. Histopathologic evaluation reveals foamy cytoplasm (with hematoxylin and eosin) This specimen is found to be oil-red-o positive, consistent with sebaceous carcinoma. *note* Sebaceous carcinomas may occur several years before a gastrointestinal malignancy. This occurrence has been described as the autosomal dominant – Muir-Torre Syndrome.
Treatment requires a resection of the malignancy. Frozen section control can be used to provide negative margins. Larger surgeries, cryodestruction and radiation may be required if resection is not possible. Exenteration (complete removal of the orbital contents is sometimes required for extensive or recurrent disease).
* Muir-Torre Syndrome: A rare, genetically autosomal dominant cancer syndrome. Patients with Muir-Torre can develop cancer of the colon, breast, genitourinary tract, skin and eye lesions, including keratoacanthomas and sebaceous carcinoma.
Melanoma of the eyelid is a relatively rare tumor making up less than 1% of eyelid cancers. However, like other skin melanomas it can spread to other parts of the body. This tumor typically appears as a pigmented thickening (tumor) of the eyelid or extension of pigment from the conjunctiva. It is characterized by a patient history of or photographically documented growth.
Symptoms
Malignant melanoma of the eyelid may look like an eyelid nevus, but it more likely to bevariably pigmented, change color, bleed and/or grow. All pigmented eyelid tumors of the eyelid should be evaluated by an eye cancer specialist.
Diagnosis
All eyelid tumors should be photographed for comparison with future examinations. if possible, patients should keep a copy of their baseline photographs. Malignant melanoma of the eyelid is distinguished from an eyelid nevus in that it can be variably pigmented, change color, bleed and/or grow. If your doctor makes a clinical diagnosis of eyelid melanoma or change is noted, the tumor should be evaluated by an incisional (not superficial) biopsy. This is because the depth of the tumor is an important risk factor for spread to the rest of the body.A simple wedge biopsy can be sent for pathologic evaluation to aid in the diagnosis. To evaluate the entire tumor, primary excisional biopsies need be performed. Once the diagnosis is made on pathology, systemic staging with total body, scalp to toes PET/CT imaging should be performed.
Treatments
When the pathology diagnosis confirms or discovers that the tumor is malignant melanoma of the eyelid (eyelid cancer), a medical work-up is ordered to stage the patient and thus rule out metastatic spread to other parts of the body. If there is no metastatic disease, the tumor can be surgically removed (including large margins of normal appearing tissue). At the time of surgery, some doctors will also remove regional lymph nodes near the tumor (in order to determine if the tumor has locally spread).
Ophthalmic plastic surgery techniques are usually required to repair the defect caused by tumor removal. The extent of surgery is governed by the ocular distribution of the tumor. That said, it can range from simple eyelid resection (wedge or Moh’s) to removal of the eyelid, debulking the orbit, to orbital exenteration. Radiation (external beam or brachytherapy implant) may be added if surgical margins are not possible.Most all patients can be repaired using one of these techniques (see Treatment Types Section).
Seborrheic keratosis is one of the most frequently noted benign eyelid tumors.
Symptoms
This is a superficial brown to black, cobble-stone surfaced tumor. Note its “stuck-on” appearance, its cobblestone surface, well-defined margins and lack of inflammation. Histopathology reveals a hyperkeratotic tumor consisting of a basaloid proliferation with keratin cysts.
Unlike squamous carcinomas of the eyelid, seborrheic keratosis does not typically cause inflammation around its edges nor does it have a smooth reddened scaly surface. If it does become inflamed it can be mistaken for a basal or squamous cell carcinoma.
Diagnosis
Typical appearing seborrheic keratosis can be photographed and followed for evidence of change prior to consideration of biopsy or removal. Suspicious seborrheic keratosis can be differentiated from other eyelid tumors by a simple biopsy.
Treatments
Seborrheic keratosis does not require treatment. Photography should be used to document its initial size for future reference and comparison. Suspicious lesions should be biopsied or removed to differentiate them from malignant eyelid tumors.
Note its “stuck-on” appearance, its cobblestone surface, well-defined margins and lack of inflammation. Histopathology reveals a hyperkeratotic tumor consisting of a basaloid proliferation with keratin cysts.
A nevus (a benign tumor) is commonly found on the skin of other parts of the human body. A nevus can also occur on the eyelid skin. These tumors are usually pigmented and have thickness.
Symptoms
Note the relatively smooth surface, no eyelash loss, a long history of its presence, and no history of recent growth. Nevi can be melanotic “dark” like this one, or amelanotic “light-colored.” *Note* Some nevi grow during puberty.
Patients typically notice a dark spot on their eyelid that is thickened. It usually does not cause loss of eyelashes and though it can grow, most do not. When rapid (over months) growth, loss of eyelashes or discoloration of the nevus is noted, malignant melanoma is suspected.
Diagnosis
Most eyelid nevi can be diagnosed by clinical examination. A baseline photograph should be obtained for comparison with future examinations. Very suspicious or rapidly growing eyelid nevi should be biopsied to rule out melanoma. It is important to note that eyelid nevi can slowly grow, and that change is particularly common during puberty.
Treatments
Eyelid nevi are benign tumors. They can be photographed and followed for evidence of change or growth prior to consideration of biopsy or treatment. Large eyelid nevi can be a cosmetic problem that can be repaired by ophthalmic plastic surgery.
The benign eyelid tumor hydrocystoma comes from the Latin hydro, meaning fluid, and cystoma, meaning cyst or sac.
A hydrocystic thickening is an epithelial-lined serous cyst (within the skin or soft tissues). Sometimes it looks like they are translucent.
Symptoms
An intradermal epithelial-lined serous cyst.
Hydrocystomas most commonly occur on the eyelids. They typically are the same color as eyelid skin, rounded and soft to the touch. They are slow growing, may cause misdirection but not loss of eyelashes.
Diagnosis
Hydrocystoma is a benign tumor that can be photographed and followed for evidence of growth. High-frequency ultrasound can demonstrate that the tumor is filled with fluid and confirm the diagnosis.
Treatments
Excision is typically performed if growth is documented, basal cell or other eyelid cancer is suspected and for cosmetic reasons. During removal, your surgeon will try and keep the cyst intact. Removing the whole tumor will help keep it from recurring.
These tumors typically grow and then spontaneously decrease in size.
Congenital “strawberry-spot” which usually will spontaneously get smaller “involute.”
Treatment is indicated for the prevention of amblyopia (loss of vision) and strabismus (misdirected eyes). These tumors naturally grow and then spontaneously decrease in size. Therefore, if the tumor is not harming the child, it can be observed untreated for spontaneous regression.
Symptoms
Capillary hemangiomas are typically found at birth. They will grow during the first decade (10 years) and most will shrink (involute). If they involve the eyelids, they can cover the eye and cause loss of vision (amblyopia). It is very important that children with capillary hemangiomas be seen by a pediatric ophthalmologist and eye cancer specialist immediately.
Diagnosis
Capillary hemangioma is diagnosed by clinical examination. It has a typical appearance and biopsy is rarely needed. It appears as a reddish tumor or mass beneath the skin. The eye care specialist will order a radiographic scan (MRI or CT) to see how deep the tumor extends into the orbit (around the eye). The child’s pediatrician should be advised and the child inspected for hemangiomas on other parts of the body.
Treatments
Observation for spontaneous resolution is commonly performed. If the tumor is blocking the eye and vision causing amblyopia, then it can be treated with an oral beta-blocker medication (e.g. propranolol) or injected with a steroid solution. This will shrink the tumor in an effort to uncover the eye. Surgery may be required to remove very large tumors. The child’s pediatric ophthalmologist may suggest that the other “good” eye be periodically covered with a patch to strengthen the tumor affected eye and prevent amblyopia-related vision loss.
A basal cell carcinoma anterior to the medial canthus: Note the pearly margins and the central crater.
The most common type of eyelid cancer is basal cell carcinoma. Most basal cell carcinomas can be removed with surgery. However, many older patients will try to ignore these slow growing tumors. However, it is important to know that when leftuntreated, these tumors can grow around the eye and into the orbit, sinuses and brain. Basal cell carcinomas are more commonly found on the lower eyelids and almost never spread to other parts of the body (metastasize).
Symptoms
Patients with basal cell carcinomas most commonly notice a reddish nodule slowly forming on their eyelid. The tumor is most commonly found on the lower eyelid, followed by the medial canthus (skin toward the nose) and can occur on the upper eyelid. Eyelash loss (around the tumor) suggests that a basal cell carcinoma is malignant.
Less commonly, basal cell cancers can be pigmented or present without any nodule at all. When the tumor does not make a nodule and grows within the eyelid, it can induce pulling of the eyelid (away from the eye). Doctors call this form of basal cell carcinoma “morpheaform,” which are much more difficult to cure because its edges are harder to define.
Diagnosis
Though small tumors can be photographed and followed for evidence of growth (prior to biopsy); once your eye cancer specialist suspects basal cell carcinoma, most eye cancer specialists will suggest tumor biopsy. This specimen is sent to the pathologist to confirm the diagnosis prior to complete removal or treatment of the tumor. Biopsies can be performed in the doctor’s office, or in the operating room prior to definitive treatment.
Treatments
Once the diagnosis is confirmed by the pathologist, treatment will be recommended. Wedge resection and Moh’s surgery require the surgeon continue to remove the tumor until the margins (edges) are negative (free of tumor). Unlike most skin, the eyelid are a complex functional apparatus that requires special reconstruction techniques.
Most basal cell carcinomas are cured when they are small. Unfortunately, some patients choose to ignore or deny the existence of these tumors. Those patients allow their tumor to invade behind the eye and become difficult or impossible to remove. In these cases, combinations of surgery, radiation and chemotherapy may be required to control or destroy the tumor.
Additional Info
This is a sun related cancer. Dr. Finger suggests, “Think of sunglasses as sunblock for your eyes”™
Tumors of the eyelids may be benign cysts, inflammations (styes), or malignant tumors (skin cancers). The most common type of eyelid cancer is basal cell carcinoma. Most basal cell carcinomas can be removed with surgery. If left untreated, these tumors can grow around the eye and into the orbit, sinuses and brain. Other eyelid cancers include squamous cell carcinoma, sebaceous cell carcinoma, and malignant melanoma. Together, these tumors make up the remaining 10% of eyelid malignancies.
Symptoms
Most patients with eyelid tumors will notice a nodular growth on their eyelid. This growth can be skin colored, red, brown or black. Malignant tumors may cause loss of eyelashes or distort the position of the eyelid. All patients with eyelid tumors should be evaluated by an eye care specialist with experience in the care of eyelid tumors.
Diagnosis
A simple biopsy can determine if an eyelid tumor is malignant.
Treatments
Malignant tumors are completely removed and the eyelid is repaired using plastic surgery techniques. Some doctors are now using topical immunotherapy or chemotherapy agents to avoid surgery. Dr. Finger can sometime use “Finger-tip” cryotherapy (freezing-therapy) or radiation therapy, depending on the extent of the tumor.
Additional info
A Typical Work-up for a Suspected Malignant Eyelid Tumor:
General: The goal should be total removal of the eyelid cancer. This usually involves primary excision with either frozen section control or the Moh’s technique.
Small tumors are usually removed by pentagonal wedge resection.
Medium-sized tumors often require reconstruction with transpositional flaps (Tenzel, Mustarde, Glabellar).
Large-tumor resections are typically reconstructed with Hughes, Hewes or Cutler-Beard Techniques.
Patient Stories
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.