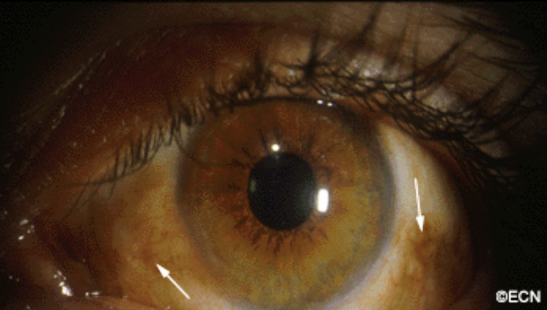
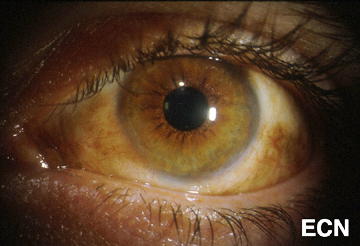
Malignant melanomas can start as a nevus/freckle or arise as newly formed conjunctival pigmentation called primary acquired melanosis (PAM).
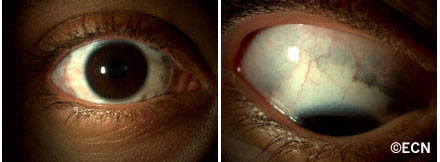
A simple biopsy can determine whether a pigmented conjunctival tumor is a nevus, primary acquired melanosis, or conjunctival melanoma. As seen below, primary acquired melanosis typically affects one eye, in middle-aged, fair-skinned people.
In contrast, darkly pigmented individuals often have naturally occurring pigment on their conjunctiva. When this occurs it is called racial melanosis. Unlike primary acquired melanosis, racial melanosis tends to involve both eyes and is typically present for the entire life of the patient.A simple biopsy can determine whether a pigmented conjunctival tumor is a nevus, primary acquired melanosis, or conjunctival melanoma. As seen above, primary acquired melanosis typically affects one eye, in middle-aged, fair-skinned people.
Symptoms
Pigmentation of the surface of the eye and/or eyelids.
Diagnosis
Most pigmented spots on the eye are benign. Your eye care specialist can take a photograph of them and watch to see if they change prior to consideration of biopsy or treatment.
Pigmented conjunctival tumors that are raised, hypervascular, or extend onto the cornea are considered suspicious. Though suspicious conjunctival tumors can be biopsied after your first visit to the eye cancer specialist, close observation for evidence of growth (prior to biopsy) may also be recommended. Documented tumor growth is a strong indicator that biopsy should be performed.
Once the biopsy is performed, the specimen should be evaluated by an ophthalmic pathologist. If there is no ophthalmic pathologist at your center, the slides can be sent for second opinion.
A pigmented conjunctival nevus can be photographed and followed for evidence of growth prior to biopsy or excision. It is important to note that both benign and malignant tumors can grow (though malignant tumors will grow faster).
Slit-lamp photography of benign conjunctival lesions is helpful in determining if subsequent change has occurred. It is a good idea for the patient to have a copy of the initial photograph because doctors are not required to keep medical records indefinitely, and the lesion can change even years after the initial diagnosis.
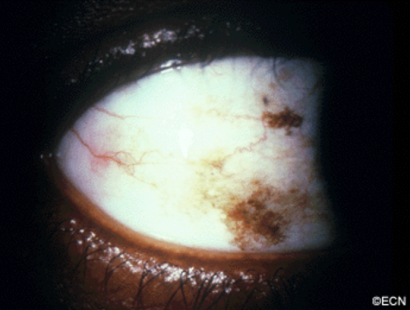
Primary acquired melanosis with atypia (biopsy proven).
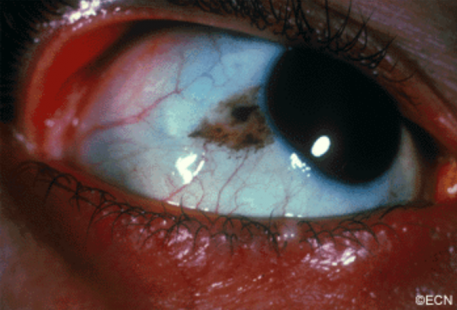
Malignant melanoma can occur on the surface of the eye (conjunctiva and cornea). It can start on its own, as a pre-existing nevus or arise within newly formed pigmentation.
Symptoms
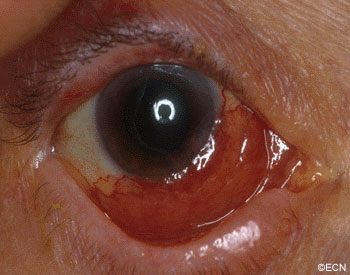
Most patients notice either a nodule forming on, or a darkening of the surface of the eye. Large tumors can bleed resulting in “bloody tears.” The tumor can extend onto the eyelid skin and lymph nodes in front of the ear (preauricular) or neck (cervical). Involved lymph nodes enlarge and can be felt (palpable) during examination.
Diagnosis
The doctor will examine your eyes. This includes an examination of all the conjunctival surfaces (including the inside of the eyelids). Pigmented conjunctival tumors are considered suspicious if they have large blood vessels running toward them, if they extend onto the cornea or if they extend into the conjunctival fornices.
Photographs should be taken of all the conjunctival and corneal surfaces at the time of initial examination (prior to any biopsy). This is important because it helps the doctor document the extent of the condition (stage the tumor) and can be used to plan for surgery and aid in follow up. Removing a conjunctival melanoma prior photography and/or referral to an eye cancer specialist can decrease the patients chance for cure.
Biopsy can determine whether a pigmented conjunctival tumor is a nevus, primary acquired melanosis, or conjunctival melanoma. A conjunctival nevus and benign acquired melanosis can be photographed and followed for evidence of change prior to intervention. Malignant conjunctival melanoma and intra-epithelial melanoma (in situ) should be removed or destroyed.
*Note* In a multicenter international effort to develop a staging system for conjunctival melanoma, the authors agreed that the term Primary acquired melanosis with atypia should be abandoned in favor of conjunctival melanoma in situ.
Treatments
Most very small areas of conjunctival hyperpigmentation can be photographed and followed for evidence of growth or change prior to treatment. If they are raised, hypervascular or extend onto the cornea a biopsy is reasonable. Small tumors can be completely removed, and if they are found to be malignant additional cryotherapy (freezing) or adjuvant topical chemotherapy may be necessary.
Melanomas can be difficult to treat if they occur at multiple spots on the eye. In these cases, surgical removal with freezing therapy may not control this tumor. Then chemotherapy eye-drops can be used for patients with conjunctival melanoma. Chemotherapy eye drops treat the entire surface of the eye, and is less dependent upon defining the tumors edges.
Lymphoma can occur in the conjunctiva. These tumors typically look like “salmon-patches.” Red colored tumors on the eye can be a presenting sign of systemic lymphoma. Eye cancer specialists usually biopsy lymphoid tumors and the pathologist is requested to perform special immunologic and genetic studies on the tumor cells. These techniques are used to determine if the tumor is benign or malignant as well as define the subtype of lymphoid malignancy.
Symptoms
The “Salmon-Patch” of Conjunctival Lymphoma.
Most patients notice the reddish discoloration of the surface of the eyeball (conjunctiva). As the tumor enlarges, patients seek medical attention. Conjunctival lymphomas can become large enough to displace the eyeball, and restrict eye movement. Eye movement restriction can cause diplopia (double-vision).
If the tumor extends behind the eyeball, it can be pushed forward (proptosis). Rarely, and if large enough, orbital lymphoma can press on the optic nerve and cause loss of vision. If discovered early, prompt treatment offers the best chance for recovery of vision.
Diagnosis
Pathology analysis of biopsied tissue allows your eye cancer specialist to determine if thelymphoma is a less aggressive MALT (mucosa associated lymphoid tissue) or the more malignant-behaving non-MALT lymphomas. Clinical differentiation between these types of cancers can be difficult.
In either case, patients with lymphoid conjunctival tumors (ocular adnexal lymphoma) should have a complete medical check up and be followed by both their eye cancer specialist and a hematologist-oncologist.
Treatments
Treatment depends on whether or not systemic lymphoma is detected. If the patient is found to have systemic lymphoma, they are likely to receive systemic immunotherapy or chemotherapy, no additional eye treatment may be necessary. However, if the conjunctival tumor is the only site of disease, most patients with malignant conjunctival lymphoma at The New York Eye Cancer Center are treated with low dose external beam radiation therapy.
This epibulbar dermolipoma is found to infiltrate the peripheral cornea and extend back to the lacrimal gland.
Epibulbar dermoids are benign tumors. They tend to be firm, white-yellow or pinkish tumors straddling the limbus in the temporal (primarily inferotemporal) quadrants. They are located both over the cornea and sclera. They can range from several millimeters to over a centimeter in size. They are typically unilateral (found on one eye), but can be bilateral.
Dermoids are choristomas (normal tissues that are in the wrong place). Made up of cutaneous and subcutaneous tissue, it is not uncommon for dermoids to contain hair and other skin structures. These tumors can be found on the eye, adnexa and orbit.
Dermolipomas are more commonly found in the superotemporal quadrant extending to the lacrimal gland and/or orbit.
Symptoms
Most patients with epibulbar dermoid or dermolipomas have no symptoms unless hairs or other dermal structures cause local irritation. The lesions do cause a cosmetic defect.
Diagnosis
The diagnosis of dermoid and dermolipoma is made by ophthalmic examination. These lesions are typically present at birth and do not progress. Though ultrasound and radiographic imaging may be required to investigate the extent of the tumor, biopsy is not necessary.
Dermoids or dermolipomas are more likely to be associated with Goldenhar’s Syndrome if they are multiple or bilateral. Goldenhar Syndrome is associated with dermoid tumors at the tragus of the ear and facial dysostosis.
Treatments
It is very important to make sure your child does not have a secondary astigmatism related to corneal tumor involvement. Early treatment of astigmatism can prevent amblyopia (loss of vision).
Surgery can be performed to limit the cosmetic defect, but there are many reports of secondary complications related to thinning of the scleral “eye wall” and corneal astigmatism.
Surgical removal of dermolipomas (that can extend into the lacrimal gland and orbit) can be associated with lacrimal gland dysfunction (dry eye) and double vision. Care must be taken to preserve the overlying conjunctiva and lacrimal gland.
Additional Info
Dermoids and dermolipomas can be associated with Goldenhar Syndrome or Linear Nevus Sebaceous Syndrome.
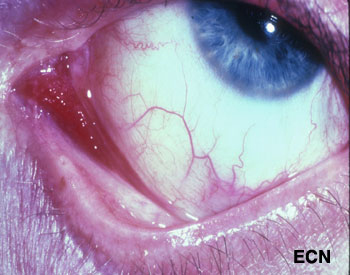
Slit-lamp photograph of a Kaposi’s sarcoma affecting the medial aspect of the conjunctiva into the fornix (arrow).
Kaposi’s sarcoma (KS) can affect the conjunctiva and eyelids. It is a red to pink conjunctival tumor and a blue to purple eyelid tumor. In North America, it is typically found in patients with HIV acquired immunodeficiency syndrome (AIDS), but can occur in the elderly and immunocompromised (e.g. transplant patients). Classic Kaposi’s sarcoma also occurs in the elderly and is slowly progressive.
Diagnosis
If the doctor suspects that a conjunctival tumor is Kaposi’s sarcoma, the patient’s skin and lymph nodes should be examined. Blood should be tested for HIV, lymphocytes, and other opportunistic diseases. One can make a tissue diagnosis based on a biopsy, or a presumptive diagnosis in patients with a history of Kaposi’s. One problem with a presumptive diagnosis (in this group of patients) is that these patients are particularly vulnerable to developing squamous and lymphoid conjunctival tumors.
Your eye care professional is more likely to suggest an incisional biopsy for diagnosis. In most cases, this can be performed in a treatment room with local anesthetic. Sterile technique, HIV precautions, and proper labeling of the specimen are required. In order to biopsy, it is not necessary to completely excise the Kaposi’s sarcoma (unless it is small and unifocal).
Treatments
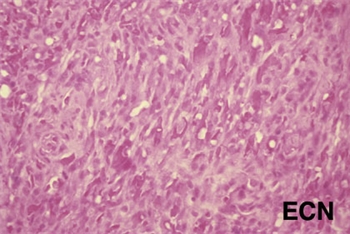
Histopathology of the excised Kaposi’s sarcoma reveals myriads of vascular channels.
Treatment depends on the patient’s age, and the status of his or her general health, current medications and immune status. Small Kaposi’s sarcomas can be removed at biopsy. Larger and multifocal tumors are biopsied, proven Kaposi’s sarcoma by pathologic analysis, and treated (systemically or regionally).
Chemotherapy, radiation therapy and biologic therapy can be employed. In cases of HIV-AIDS related Kaposi’s sarcoma, we tend to avoid any treatment that would further suppress the patient’s immune system. If treatment of the patient’s underlying HIV-AIDS does not halt the progression of the Kaposi’s sarcoma, this tumor has been found to be very sensitive to external beam radiation therapy.
Additional Info
For the ophthalmologist who discovers conjunctival Kaposi’s sarcoma, it is important to coordinate care with a team consisting of a medical oncologist (and/or HIV-specialist), and radiation oncologist.
Malignant cancers can grow on the surface of the eye. They usually start from the membrane that covers most of the eye called the conjunctiva. The most common conjunctival cancers are squamous carcinoma, malignant melanoma and lymphoma.
Malignant melanoma used to be called PAM with atypia, but the newest AJCC staging system authors suggest we stop using the term PAM with atypia and call it melanoma in situ. This was because PAM with atypia doesn’t define it as a cancer. Pathologists call these specimens Tumor in situ or Tis.
Squamous carcinoma of the conjunctiva can form a nodule or diffusely spread out over the surface of the eye. Only very large squamous conjunctival cancers and those in patients who are immunosuppressed metastasize to other parts of the body. But they can invade into and around the eye, into the orbit and sinuses.
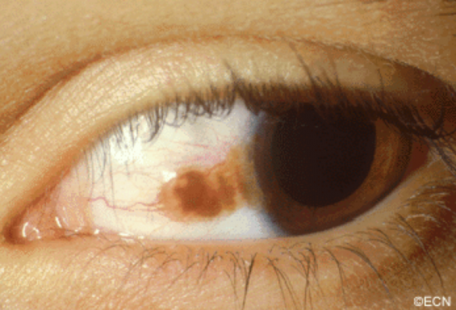
Malignant melanoma can start as a conjunctival nevus, arise as newly formed pigmentation (or variably pigmented) within the conjunctiva or onto the cornea. A simple biopsy can determine whether a pigmented conjunctival tumor is a benign nevus, primary acquired melanosis, or conjunctival melanoma.
Lymphoma can also occur in the conjunctiva. These tumors look like red or salmon-colored patches on the eye and can be the first sign of systemic lymphoma. Eye cancer specialists usually biopsy lymphoid tumors so that a pathologist can perform special immunologic and genetic studies on the tumor cells. These techniques are used to determine if the tumor is benign or malignant. Patients with lymphoid conjunctival tumors should have a complete medical check up and be examined by a hematologist-oncologist. Other “less common” conjunctival cancers are reviewed in this section.
Symptoms
Most conjunctival tumors do not cause symptoms. Patients typically seek medical attention because they notice a discoloration on the eye or extension of the tumor onto the cornea. Conjunctival tumors can also be found by an eye care specialist during a routine eye examination.
Diagnosis
Most small benign-appearing conjunctival tumors can be photographed and followed for evidence of growth prior to biopsy or treatment. If they are raised, hypervascular or extend onto the cornea a biopsy is more reasonable. At The New York Eye Cancer Center we typically obtain an office-based cytology specimen for squamous carcinoma. This lets us know the tumor is squamous and avoids a trip to the operating room. In contrast, both melanoma and lymphoma require more histopathology and special pathology analysis. Therefore, those tumors require surgical biopsy or if small, excision.
Conjunctival melanomas require special treatment. The natural history of these tumors has been characterized as presenting with multiple tumors or non-pigmented skip areas.
Therefore, it is difficult and some think impossible to define the extent of the tumor on clinical examination.
The So-Called “No Touch Technique”
The natural skip areas of pigmentation, multifocal presentation and high rates of recurrence have led some eye cancer specialists think that handling conjunctival melanoma promotes spread. They fear that tumor cells get stuck on the instruments that if reused, implant tumor on other, unaffected parts of the globe.
However, Dr. Finger disagrees with this theory and its so called “no touch technique” that requires surgeons to get new instruments after each time they touch the tumor (to prevent transplantation). However, there are no other cancers where surgeon-related transplantation has been found. More likely, these eye cancer specialists operate on one area, thinking that the pigmented portion of the tumor is the complete extent of disease. Unaware, there are other non-pigmented or small tumors that are not yet visible and later grow. Then they think they transplanted the tumor.
At The New York Eye Cancer Center, when conjunctival melanoma is suspected, Dr. Finger utilizes his specially designed cryotherapy devices “Finger-tip” cryotherapy probes” to make sure the tumor and a surround of normal appearing tissue is treated before he touches the tumor. Then the tumor can be safely removed without fear of transporting tumor cells or invaginating the edges of the wound rendering tumor too deep to treat with chemotherapy eye drops. At The New York Eye Cancer Center, topical chemotherapy eye drops are used for treatment of both squamous and melanoma cancers. These drops have been found to reduce or more commonly eliminate the need for extensive surgery.
Evaluation of the biopsy specimen should be performed by an experienced ophthalmic pathologist. If there isn’t an ophthalmic pathologist in your area, you can request that the histopathology slides be sent for second opinion.
Treatment: General Guidelines
Small tumors can be completely removed, and if they are found to be either squamous carcinoma or malignant melanoma, additional cryotherapy (freezing) is likely to improve local tumor destruction and thus prevent recurrence. Dr. Finger has developed specialized “Finger-tip” cryotherapy probes to uniformly freeze large surfaces of the eye with minimal intraocular penetration (see innovations section).
Chemotherapy Eye Drops:
Conjunctival melanoma and squamous carcinoma can be difficult to treat if they are “mulitfocal” – occur in multiple spots on the eye. In these cases, even surgical removal with freezing therapy may not control the tumor. Dr. Finger has found that “Chemotherapy eye-drops can be used for and are often better than surgery for most patients with conjunctival cancers.” Chemotherapy eye-drops treat the entire surface of the eye, are less dependent upon defining the tumors edges, and decreases the chance of scarring (symblepharon) after surgery. Researchers at The New York Eye Cancer Center recently published on treatment of “Giant Conjunctival Squamous Carcinoma’ with chemotherapy eye drops alone (no surgery).
Systemic lymphoma can usually be treated with standard chemotherapy that is also likely to cure malignant ocular lymphomas. If the eye is the only site of malignant lymphoma, low dose external beam radiation therapy is commonly employed.
Note the increased pigmentation of the eyelid and episclera. This patient was also noted to have heterochromia (different colored irides) and a darker fundus (more pigment in the choroid) by ophthalmoscopy.
Patients with the Nevus of Ota have increased amounts of melanin (pigment) and melanin producing cells (melanocytes) in and around their eyes. This includes the intraocular blood vessel layer called the uvea (choroid, ciliary body, and iris), on the white part of the eye ball (sclera), and in the eyelids.
Patients with the Nevus of Ota have been shown to be at greater risk for the development of intraocular and central nervous system malignant melanomas (e.g. choroidal melanoma). Though intraocular melanomas are more common in these patients, their lifetime risk is though to be 4%.
Patients with the Nevus of Ota should be examined at least every 6 months by an eye-cancer specialist and a neurologist.
Symptoms
The Nevus of Ota appears as increased pigmentation of one eye and its eyelids. The eyelid is darkened, pigment can be observed on the white of the eye and that iris may be darker (compared to the contralateral iris). Though none of these findings produces physical symptoms, physical asymmetry can have a psychological impact on the patient.
Ocular Melanosis is diagnosed in cases of ocular melanosis there is no eyelid involvement.
Diagnosis
Ocular Melanosis: Episcleral and uveal hyperpigmentation without eyelid skin involvement is called “Ocular Melanosis”
Careful inspection of any patient with two different colored irises (heterochromia irides) may uncover the eyelid and episcleral pigmentation diagnostic of the Nevus of Ota.
Slit-lamp biomicroscopy is used to distinguish between conjunctival and episcleral pigmentation. Comparative examination of the irides can be used to evaluate coloration and surface characteristics.
Dilated ophthalmoscopy similarly demonstrates asymmetric “darker” pigmentation of the choroidal vascular layer beneath one retina.
Ophthalmic ultrasound imaging will reveal thickening of the vascular uveal layer of the eye. Examinations should include both posterior and anterior segment (UBM) imaging.
Treatments
Most patients with the Nevus of Ota have no subsequent related problems.
Less than 4% can develop choroidal melanoma in the affected eye. Fewer will develop intracranial neoplasia. Therefore, it is reasonable for all patients with the Nevus of Ota to have twice yearly eye examinations with dilated ophthalmoscopy. They should also have an initial neurology assessment, followed by periodic medical evaluations.
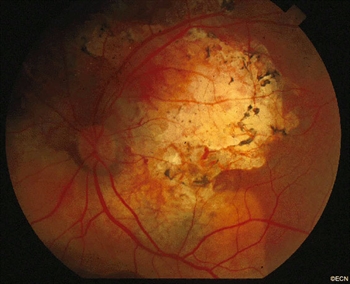
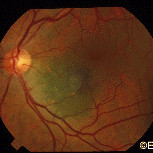
Choroidal Osteoma: Note that the tumor surrounds the optic nerve and it has a relatively light color. There is pigment over the tumor surface and it has scalloped edges. In this case (and at this time) no subretinal neovascularization is present.
Choroidal osteoma are boney tumors that can grow within the eye. They arise within the blood-vessel layer “choroid” beneath the retina. Choroidal osteoma are usually found near the optic nerve and can cause vision loss. The choroidal osteoma impedes the circulation to (and harms) the overlying retina and can be associated with overlying retinal atrophy and adjacent subretinal neovascularization (or, the formation of new blood vessels).
Symptoms
Most choroidal osteomas do not cause any symptoms. They are found on routine eye examination. However, they can be associated with the development of subretinal neovascularization (particularly at the edges of the osteoma). If in the center of the macula, the blood and neovascularization can cause distortion or loss of vision.
Diagnosis
A choroidal osteoma is characterized by bone in the choroidal vascular layer of the eye. These bone deposits are more likely to be found near to the optic nerve, and they are relatively flat (typically less than 2 mm thick). By looking into the eye (i.e., performing an ophthalmoscopy), your doctor will see the yellow tumors, scalloped edges, formed vessels within the tumor, some pigment clumping on its surface, and, rarely, blood associated adjacent subretinal neovascularization.
In the adult or peripheral form of the disease, the doctor might just see the tumor eroding through the overlying retinal pigment epithelium like the tip of an iceberg. In these cases, the extent of the base of the tumor might only be measured by ultrasound imaging.
Photography is used to document the choroidal osteoma size and shape. Baseline photographs are helpful for subsequent evaluations for growth and neovascularization.
A few tests additional tests may be performed in order to confirm diagnosis:
Fluorescein angiography: Since a choroidal osteoma is made of bone, when fluorescein dye circulates through the eye, it will be slow to penetrate the tumor. Once the fluorescein dye is inside the choroidal osteoma, it also has trouble getting out. This is why the fluorescein pattern of choroidal osteoma is one of slow uptake and persistent “late” fluorescence.
Ultrasound: Ultrasound examination of an eye with a choroidal osteoma will demonstrate intense reflectivity from the hard bony tumor with resultant shadowing of the posterior orbital contents. If the intensity (gain) of the ultrasound machine is decreased, the eye-care specialist is likely to see persistentm characteristic very high reflectivity or “brightness” from the tumor. Ultrasound can also be used to measure the thickness of a choroidal osteoma.
Radiographic imaging: Computed tomography (CT) can be particularly helpful to see the calcification of a choroidal osteoma in unusual cases.
Treatments
Choroidal osteoma is a benign tumor; therefore, most patients do not require treatment. Choroidal osteoma related vision loss is not usually treatable. On occasion, a choroidal osteoma may be associated with subretinal neovascularization (abnormal blood vessels beneath the retina), which are typically treated with laser.When these abnormal vessels are on top of the tumor or near the central vision, intraocular anti-VEGF drugs may be advised.
Eye tumor specialists request that choroidal osteoma is monitored with periodic dilated ophthalmoscopic examinations.
Like a raised freckle on the skin, nevi can also occur inside your eye. The most common “choroidal nevus” or eye nevus are unusual and can only be seen by an eye care specialist. Like a nevus on the skin, a choroidal nevus can grow into a malignant melanoma.
A choroidal nevus rarely requires treatment. Photography is typically used to document the size of the choroidal nevus. If the choroidal nevus has orange pigmentation, if the nevus is leaking fluid, or has a thickness of 2 mm or more it may be (or become) a malignant choroidal melanoma.
Depending on its appearance, patients with a choroidal nevus should have their eyes examined (at least) every 6 months. Only your doctor can look inside your eye to see if the choroidal nevus has changed. If the choroidal nevus has orange pigment or has thickened, it should be checked more often. If a choroidal nevus is leaking subretinal fluid, this is a particularly ominous sign. Such tumors should be followed most closely for evidence of growth or malignant transformation into a choroidal melanoma.
It is reasonable to have an eye cancer specialist check to see if your choroidal nevus looks suspicious and take baseline measurements. This examination may include the use of ultrasound, specialized photography, optical coherence tomography or an intraocular angiogram. It is a good idea for each patient to keep a picture of your choroidal nevus. This picture can be compared to future examinations to help determine if the nevus has changed or stayed the same.
Symptoms
A benign choroidal nevus (eye freckle) rarely causes symptoms. However, if a choroidal nevus leaks fluid or is associated with the growth of abnormal blood vessels (neovascularization) patients can become symptomatic. Such changes can cause a localized retinal detachment/degeneration, flashing lights and loss of vision.
A typical choroidal nevus is asymptomatic or “causes no symptoms” and found by routine dilated eye examination with ophthalmoscopy.
Diagnosis
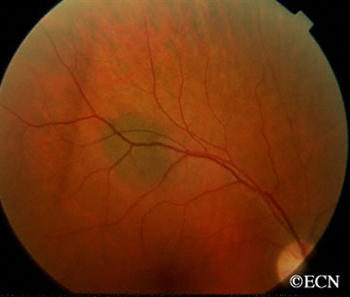
This image demonstrates how a suspicious choroidal nevus can demonstrate focal leakage on fluorescein angiography.
Choroidal nevus is typically a pigmented tumor of the blood vessel layer (choroid) beneath the retina. A choroidal nevus is typically gray but can be brown, yellow or variably pigmented. Your eye care professional will look to see if the choroidal nevus is raised (has thickness), orange pigment (lipofuscin), or is leaking fluid (retinal detachment). If the choroidal nevus has one or more of these findings, it is labeled a suspicious choroidal nevus that has a chance of turning into or even being a small choroidal melanoma.
A choroidal nevus can have yellow-white spots on its surface called drusen or drusenoid retinal pigment epithelial detachments (DRPED).These are signs of retinal dysfunction. The nevus may be preventing the eye from removing retinal waste products or creating microscopic leaks beneath the retina.There are no studies that show how long it takes for drusen to form on a choroidal nevus.
Treatments
A benign choroidal nevus requires no treatment and there is no way to safely remove them. Since a choroidal nevus can turn into a choroidal melanoma, it is reasonable to have it periodically observed by your eye care professional.
Additional Info
Dr. Finger believes that since skin and conjunctival melanomas have been linked to ultraviolet exposure, and since choroidal melanomas are more commonly found in patients with blue eyes, outdoor occupations, and in Australia (where there is an ozone hole); it is reasonable to wear ultraviolet (UV) blocking sunglasses. Dr. Finger says, “Think of sunglasses as sun block for your eyes.”™
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.