Circumpapillary Metastasis with Optic Neuropathy
By Paul T. Finger, MD
Description
Malignant tumors from other parts of the body can spread in and around the eye. These tumors may never be discovered unless they affect the vision, are visible in the iris, or push the eye forward.

Symptoms
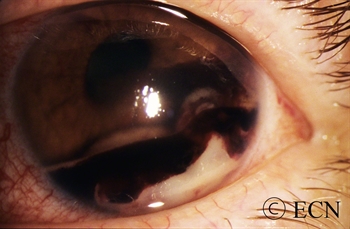
Most patients with choroidal metastasis have no symptoms, that is unless the tumor affects the central macular retina, optic nerve or the front of the eye (iris). For example, this patient’s tumor (pictured above) affected his optic nerve, caused decreased vision and floaters (spots in his vision).
Diagnosis
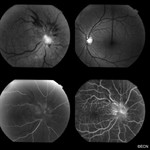
Most patients have a history of primary cancer (as in this case), and the tumor’s characteristics are typical of metastatic disease. This tumor was yellow-white, poorly circumscribed, less than 3 mm thick and causing congestion with vascular compromise of the optic nerve.
Treatments
As with this patient, most choroidal metastasis will resolve with external beam radiation therapy. Like many patients treated for metastatic disease, this patient received 30 Gy in 10 daily fractions. Other treatment protocols (doses) may be different, depending on the type of primary tumor.
Dr. Finger currently recommends that orbital radiation therapy for metastatic disease be performed in 180-200 cGy daily fractions. This is due to the unique sensitivity of the eye and lacrimal (tear) systems. With improvements in systemic therapy, patients are living longer and thus developing late radiation complications. Dr. Finger believes these complications will be less likely if the radiation is delivered in smaller daily fractions.