A relatively new treatment for retinoblastoma quickly gaining popularity has shown some promise, but a systematic review of reported outcomes published in March provides some reason for caution.
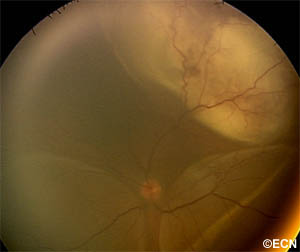
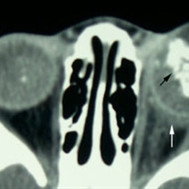
Intra-arterial chemotherapy has rapidly emerged as a treatment for intraocular retinoblastoma, the most common primary childhood eye cancer. It involves inserting a microcatheter into the ophthalmic artery and manually injecting chemotherapy drugs though it directly into the eye.

Centers in some 30 countries have adopted the technique, and a few have completely replaced systemic chemotherapy and radiation with intra-arterial chemotherapy as the primary treatment for retinoblastoma.
Last year, several doctors set out to perform a systematic review to summarize reported outcomes of intra-arterial chemotherapy. They published their results in the Journal of the American Medical Association, Ophthalmology in March, 2016.
The researchers performed comprehensive searches in Medline, Embase, Cochrane, and Web of Science from inception through January 2015. They included any peer-reviewed English-language publication that described outcomes related to toxicity or efficacy in at least four patients. Through their search, the doctors identified 28 publications that met their inclusion criteria. The researchers ultimately evaluated cases encompassing 655 patients, 757 eyes, and a total of 2,350 catheterizations.
Join Our Mailing List
While they found the treatment yielded a 66% eye-preservation rate, the number of children who subsequently developed metastases raises concern. The researchers concluded that while the treatment seems promising, more study is needed.
“Metastases have been observed, and long-term follow-up is needed. “Until the results of clinical, prospective studies are available, it is recommended that intra-arterial chemotherapy be offered selectively among other options, with fully informed discussion about all possible risks, benefits, and uncertainties.”
The researchers pointed out that the prior method of systemic chemotherapy addressed the issue of metastases, while intra-arterial chemotherapy does not.
“The most important critique of the IAC literature is the uncertain rate of metastases. Eye salvage is only valuable when achieved without a risk to life. Systemic chemotherapy provides protection against metastases, especially in children who may have unknown high-risk pathologic features in retained eyes, but IAC does not.”
While promising, intra-arterial chemotherapy may not be the panacea some doctors hope. The recently published systematic review of reported outcomes indicates some caution is necessary and more study is definitely needed.
You can read the complete study in the March 2016 issues of the JAMA Ophthalmology. Access it HERE.