Intraocular Lymphoma (Vitreoretinal Lymphoma)
By Paul T. Finger, MD
Description
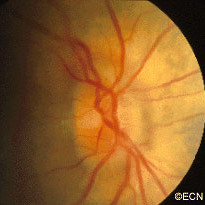
Most patients diagnosed to have intraocular lymphoma have symptoms of vitreous floaters, a history of systemic lymphoma or have been diagnosed as having chronic uveitis. Any patients with vitreous cells, no history of recent intraocular surgery and a non-painful eye should be suspected to have intraocular lymphoma.
Symptoms
Case Example: A 70-year-old woman was noted to experience an acute deterioration of her vision due to vitreous cells. A diagnostic vitrectomy was performed. Pathology showed large B-cell lymphoma. A complete metastatic survey (imaging studies of the brain, chest, abdomen), lumbar puncture and bone marrow biopsy were found to be negative.
Diagnosis
The diagnosis of intraocular lymphoma is typically made by removal of cells (vitrectomy biopsy) from the eye with subsequent cytopathologic evaluation. Lymphoma biopsy should be performed at a center with ophthalmic pathology services used to working with small specimens. Once the diagnosis is certain, a hematologist-oncologist should be consulted to perform an evaluation for systemic and central nervous system lymphoma (staging).
Treatments
Though chemotherapy can be used to treat the systemic disease, poor intraocular drug penetration can leave residual lymphoma in the eye. In these cases, external beam radiation therapy to the eyes and orbits will typically clear the intraocular disease.
The literature consists of a multitude of case-reports and no evidence based comparative studies. In my experience, most patients are eventually treated with ocular irradiation. Others have had prophylactic whole-brain irradiation as well as combinations of local and systemic chemotherapy.
What is common to most of these reports is that, when the lymphoma is found in the brain, the prognosis is poor. Clearly, a natural history study followed by prospective randomized treatment trials would be helpful to find the cure for patients with intraocular lymphoma.
Additional info
Radiation Therapy
Radiation therapy has been the most common treatment for intraocular lymphoma. Both eyes are usually treated because approximately 80% of cases will either present as or go on to develop bilateral disease (within 8 years).
The prescription dose has been decreasing with less than 3,000 cGy being employed in many centers. The dose to the orbit is adjusted when whole-brain irradiation is required. With this in mind, remember to always obtain a complete neurological work-up to rule out central nervous system (CNS) involvement. Radiation will help acutely, but intraocular and CNS relapse are common.
Chemotherapy
Recent investigations have combined radiation therapy with systemic or intrathecal chemotherapy. Several studies suggest that this approach has prolonged survival. Chemotherapeutic agents have been given intravenously, intrathecally, and intravitreally (into the eye).
Injections of chemotherapy into the eye have been investigated as an alternative to radiation. Typically using methotrexate and/or retuximab, multiple injections are required and carry the known risks associated with ocular perforation (e.g. infection) as well as chemotherapy associated side-effects. This is why most centers use intravitreal chemotherapy when patients demonstrate intraocular recurrence after failure of radiation therapy.