New Radiation Instructions for Eye Plaque Patients 2018
Based on published guidelines from United States Nuclear Regulatory Commission (NRC), The New York Eye Cancer Center and its affiliate New York Eye and Ear Infirmary of Mt. Sinai have agreed that patients undergoing low energy (iodine-125 or palladium-103) eye plaque radiation therapy for intraocular melanoma are allowed to proceed with their lives as usual.
Before this change, eye plaque patients were required to almost quarantine themselves. They had to remain at home, maintain a distance of 6-feet from others, and no pregnant women or children were allowed to visit.
With the new changes, patients can use public transportation. We ended most of the radiation exposure precautions and restrictions (i.e. you may go to the park, restaurants, grocery stores…etc.). However, it is recommended that patients stay at home as much as possible and that they do not engage in activities that could dislodge the implant and/or seeds. As before, the patient’s body fluids, clothing, and utensils ARE NOT radioactive and can be handled by others safely. We ask that the patient sleep alone and in a separate room away from anyone under the age of eighteen.
Dr. Finger says it’s about time: “With the radiation implants I use, eye cancer patients typically receive only a small fraction of the radiation given to patients undergoing implant radiation for other cancers, where patients are sent home on the day of implant.”
Though a few rules remain, they new radiation instructions are not nearly as strict. Free at last, patients can feel the sunlight, do their own shopping, and enjoy the company of their loved ones.
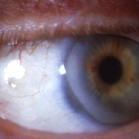
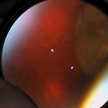
External photograph shows the pigmented tumor “melanoma” in the conjunctiva.
By Paul T. Finger, MD
Current treatments for conjunctival cancer has included surgical removal, removal with subsequent cryo-(freezing)-therapy, radiation therapy, and chemotherapy eye-drops. While most treatments have focused on avoiding large surgeries which may (in very severe cases) be associated with vision loss or loss of the eye, these decisions have been made with the knowledge that conjunctival cancers are serious. They can invade into the orbit (tissues around the eye), the sinuses, and the brain. Conjunctival melanomas and squamous carcinomas can also spread (metastasize) to other parts of the body. Because of high recurrence rates after standard treatments and the desire to avoid surgery, recent investigations have focused on topical chemotherapy “eye-drops.”
For a more detailed explanation of the risks and potential benefits of topical chemotherapy for conjunctival cancers, the editor suggests you obtain and read the referenced manuscripts.
After 28 days of topical MMC chemotherapy the tumor regressed.
Conjunctival Melanoma and PAM with Atypia
In 1993, Dr. Finger was the first to use mitomycin chemotherapy eye-drops to treat conjunctival melanoma and primary acquired melanosis. Since that time, it has become commonly and widely used throughout the world. It is currently used to reduce the tumor prior to surgical removal and with surgery for cases where there is too much normal tissue involved (too much for surgery and/or freezing (cryotherapy).
In addition, Dr. Finger discovered that topical interferon chemotherapy (Intron A) eye drops can be used to treat superficial conjunctival melanoma.
Topical chemotherapy eye drops can be used as primary treatment, as well as an addition to surgery and cryotherapy. Since almost all conjunctival tumors have different sizes, shapes and locations, your eye cancer specialist should know when and if you are a candidate for topical chemotherapy.
Squamous Conjunctival Neoplasia
Chemotherapy eye-drops have also been investigated as an alternative treatment of squamous conjunctival – corneal neoplasia. For more information consider reading the following manuscripts. Squamous Conjunctival Neoplasia
References
Finger PT, Milner MS, McCormick SA. Topical chemotherapy for conjunctival melanoma. British Journal of Ophthalmology 77:751-3, 1993
Frucht-Pery J, Pe’er J. Use of mitomycin C in the treatment of conjunctival primary acquired melanosis with atypia. The Archives of Ophthalmology 1996;114:1261-1264.
Finger PT, Czechonska G, Liarikos S. Topical mitomycin C chemotherapy for conjunctival melanoma and PAM with atypia British Journal of Ophthalmology 82:476-9, 1998
Finger PT, Sedeek RW, Chin KJ. Topical interferon alfa in the treatment of conjunctival melanoma and primary acquired melanosis complex. Am J Ophthalmol. 2008 Jan;145(1):124-129.
Danapoulos ED, Danpoulous IE, Liarikos SB et al. Effects of urea treatment in malignancies of the conjunctiva and cornea. Ophthalmologica 178:198-203, 1979
De Keizer RJW, de Wolff-Rouendaal, van Delft JL, et al. Topical application of 5-FU in premalignant lesions of the cornea, conjunctiva, and eye lid. Doc Ophthalmol 64:31-42, 1986.
Frucht-Pery J, Rozenman Y. Mitomycin C treatment for conjunctival -corneal intraepithelial neoplasia: A multicenter experience. Ophthalmology 104:2085-2093, 1997
Wilson MW, Hungerford JL, George SM, Madreperla SA. Topical mitomycin C for the treatment of conjunctival and corneal epithelial neoplasia. American Journal of Ophthalmology 124:303-311, 1997
The authors examined if the American Joint Committee on Cancer (AJCC) staging system for ocular adnexal lymphoma (OAL) could be used to predict local control and systemic disease. A multicenter, consecutive case series of patients with biopsy-proven conjunctival, orbit, eyelid, or lacrimal gland/sac lymphoma was performed.
Results
They found that extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue was the most common and AJCC clinical stages were cT1NOMO (21.7%), cT2NOMO (44.6%), cT3N0M0 (5%), and cT4NOMO (2.4%).
Treatment was able to control the local tumor in 75% of patients.
Of the 19 local recurrences, 74% (most) were found after non-radiation based treatments.
The lower-risk “smaller tumor” AJCC T1 and T2 groups without lymph node involvement or metastatic disease had longer disease-free survival than the higher-risk AJCC T1, T2 with nodal involvement or metastatic disease, AJCC T3, and T4 as well as Ann Arbor II, III, and IV.
Conclusions
Regardless of stage, recurrence and disease-free survival were more closely related to having had radiation treatment and histopathology rather than site specific factors, such as tumor size or location around or behind the eye.
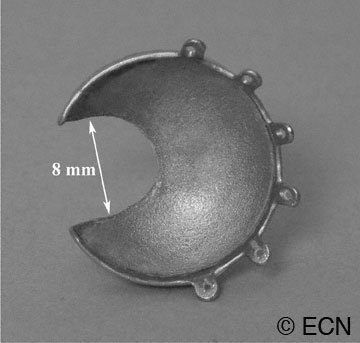
Dr. Finger invented “Slotted Eye Plaques” for treatment of juxtapapillary and circumpapillary intraocular tumors. Standard COMS-type gold eye-plaques were altered such that an 8-mm-wide (variable length) slot was created to accommodate the orbital portion of the optic nerve. As the nerve entered the slot, the plaque’s posterior margin extended beyond the optic disk as to cover tumor (on the opposite side). Radioactive seeds around the slot, surround the tumor and its posterior tumor margins.
Dr. Finger says, “due to the physical limitations of notched plaques, there was no plaque device that could extend to cover and treat the posterior portion of a tumor that came within 1.5 mm, touched or surrounded the optic nerve.” This is why Dr. Finger invented slotted eye plaques. Intraoperative ultrasound imaging is used to confirm proper plaque placement. Preoperative radiation dosimetry showed that all tumour-tissue received a minimum of 85Gy (despite the gap created by the slot). To date, there has been only one tumor regrowth which is much better than previous plaque treatments for these tumors. No new complications that might prevent the use of slotted plaque radiation therapy have been noted.
Graphic Animation of a Slotted Plaque in Position over a Circumpapillary Tumor
Dr. Finger says, “slotted plaques represent an innovation that improves radiation coverage for tumors that touch or surround the optic nerve. For the first time, this technique allows plaque radiation therapy to include the entire juxtapapillary and circumpapillary tumor within the treated zone. It “normalizes” plaque treatment of these tumors. He adds, this technique addresses the problems some centers were having with local control of tumors in this location. Certainly, it will allow more patients to keep their eyes and their vision.”
For more complete information read these manuscripts published in the British Journal of Ophthalmology and Ophthalmology in 2012 or contact Dr. Finger.
Case 1: An Iris Melanoma after DilationCase 1: An Iris Melanoma before Dilation
Notice the low reflective mass in the iris. There is thinning of the iris pigment epithelium and a length of relatively normal appearing iris between the posterior margin of the tumor and the ciliary body. In this case, the tumor was documented to grow and cataract surgery was contemplated. In part, due to these dynamic high-frequency ultrasound findings, excision was planned prior to dilation for cataract surgery.
This case illustrates that high-frequency ultrasound allowed for unique views of the posterior aspect of the tumor, as well as an assessment of its invasion within the iris stroma.
Case 2: A Sigh of Relief
Case 2: High-frequency ultrasonography demonstrates a cystic “acoustically empty” tumor displacing the iris anteriorly, causing focal angle closure.Case 2: A smooth-surfaced tumor is seen posterior to the iris stroma and anterior to the anterior lens capsule.
The iris cysts are the most common iris tumor sent for high-frequency ultrasonographic evaluation. Its clinical presentation is similar to seeing a localized “bulge” in the iris. Ultrasonography clearly demonstrates the cystic nature of the tumor and allows for an assessment of the adjacent ciliary body (for tumor).
Cases 3 & 4: A Unique tool
Image 2Image 1
This melanoma has grown through the iris pigment (image 1) epithelium onto the anterior capsular surface. High frequency ultrasonography allows for an assessment of tumor penetration of the iris and ciliary body.
This small ciliary body melanoma (image 2) would likely have gone undetected prior to high frequency ultrasonography. Like other malignant tumors, early detection and treatment of ciliary body melanomas should improve survival.
References
Reminick LR, Finger PT, Ritch R, Weiss S, Ishikawa H. Ultrasound biomicroscopy in the diagnosis and management of anterior segment tumors. Journal of the American Optometric Association 69(5);575-582, 1998.
Katz NR, Finger PT, McCormick SA, Tello C, Ritch R, Sirota M, Kranz O. Ultrasound biomicroscopy in the management of malignant melanoma of the iris. The Archives of Ophthalmology 1995;113:1462-1463.
By Paul T. Finger, MD Ophthalmic plaque brachytherapy has become the most common eye-sparing technique for the treatment of intraocular tumors. Eye plaques are constructed by affixing radioactive seeds within a gold, metallic, bowl-shaped carrier.
Then the radioactive eye plaque is sewn to the wall of the eye underneath the intraocular tumor. It is left in place for several days during which the tumor is sterilized by the radiation.
Small diode lights can be attached to ophthalmic plaques in order to improve their localization beneath their intraocular tumors and to allow photo-documentation of plaque position. With the lights turned on, we could see that the plaques were in position as to cover the intraocular tumor.
In most centers, radiation therapy has been able to destroy choroidal melanomas in over 92% of cases. Unfortunately, at least 8% of tumors have been found to regrow within 5 years of treatment. These failures of local control are thought to be due to radiation resistant tumors and to suboptimal placement of the eye-plaque (using standard transillumination techniques). This is evidenced by more failures occurring in treatment of small tumors near the optic nerve. These cases are difficult or impossible to visualize with standard transillumination or ultrasound techniques. Diode-light transillumination was invented to improve localization of eye plaques beneath these small posterior tumors.
References
Finger PT, Iezzi R, Romero J, Rosen RB, Szechter A, Hegde H. Plaque-Mounted Diode-Light Transillumination For Localization around Intraocular Tumors. The Archives of Ophthalmology 1999:117:179-183.
Finger PT, Iezzi R, Esteveo ML, Szechter A, Rosen RB, Berson A. Diode-Light Transillumination for Ophthalmic Plaque Localization around Juxtapapillary Choroidal Melanomas. The International Journal of Radiation Oncology, Biology, Physics 44:887-890, 1999.
Ten years after treatment the tumor has regressed to scar with scleral show.
Heat “Hyperthermia” has been used to make radiation more effective in the treatment of cutaneous and metastatic malignant melanoma. This is because relatively low levels of heat (42-45 Celsius) can inactivate enzymes used to repair radiation damage and higher temperatures can damage tumor blood vessels.It is believed that low level heating offers the potential to decrease the amount of radiation required to kill cancer cells resulting in fewer radiation complications.
The largest and longest followed series of patients treated with both eye-plaque radiation therapy and ocular hyperthermia was published in 1997. This phase-I clinical case series demonstrated comparable local control and improved visual acuities compared to other series of patients treated with radiation alone. For further information read, see links below.
Unfortunately, due to the small numbers of patients and commerical liability concerns/expense, hyperthermic treatment of choroidal melanoma was not found to be commercially viable. If there is commercial interest, please contact Dr. Finger.
References
An anterior choroidal melanoma prior to I-125 /microwave thermoradiotherapy.
Finger PT. Microwave thermoradiotherapy for uveal melanoma: Results of a 10-year study. Ophthalmology 1997;104:1794-1803.
Lagendijk JJ. A microwave heating technique for the hyperthermic treatment of tumours of the eye, especially retinoblastoma. Phys Med Biol 1982; 27:1313-1324.
Petrovich Z, Pike M, Astrahan MA, Luxton G, Murphree AL, Liggett PE. Episcleral plaque thermoradiotherapy of posterior uveal melanomas. Am J Clin Oncol 1996;19:207-211.
For a complete review of the methods of hyperthermic treatment for intraocular tumors read: Finger PT. Thermoradiotherapy for Eye Tumors. In: Medical Radiology – Diagnostic Imaging and Radiation Oncology, Volume 2: Principles and Practice of Thermoradiotherapy and Thermochemotherapy. Seegenschmiedt MH, Fessenden P, Vernon CC, eds. Berlin: Springer-Verlag, 1993 175-185.
Dr. Finger’s patented, expandable orbital implant will have the capacity to be enlarged as the surrounding orbital tissues atrophy. An enlarging prosthesis should help correct ptosis (drooping eyelid), enophthalmos (sunken eye) and motility (movement). Clinical trials will be needed to evaluate this effect on movement and cosmetic results for patients. The movie demonstrates the capacity of the implant to expand. In practice, the implant will be inflated and allowed to stay in its expanded state. Dr. Finger is interested in finding a company to produce this patented implant.
Advantages
They cannot become infected.
They are not made of nor contain calcium (that can affect subsequent imaging or radiation treatment). The implant sits in the orbit and behind the ocular prosthesis.
General Information About Enucleation
The expandable orbital implant has an anterior injection portal, rectus muscle placement grooves, and 4 independently expandable/deflatable quadrants.
Volume-Replacement After Enucleation
Enucleation (“removal of the eye”) is typically recommended for patients:
1. With a large intraocular eye cancer which cannot be destroyed or removed by other methods.
2. When alternative treatments are likely to leave the patient with poor or no useful vision.
3. With a blind and painful eye.
4. When a patient requests removal of the eye as treatment for their eye cancer.
Current Types of Implants
Drooping of the left upper eye lid (ptosis) Implants are used to replace the volume lost by the enucleation procedure.
When this type of implant is placed in the orbit, it is surrounded by the extraocular muscles and soft tissues. After it heals, the prosthesis (which looks much like a giant contact lens) is placed over the implanted ball. The ball-muscle complex functions much like the ball in a ball-in-socket joint. Therefore, when the implant moves, the overlying prosthesis also moves.
Non-integrated implants:
The implant sits in the orbit and behind the ocular prosthesis.
The can be made of glass, PMMA, silicone (PMMA plastic is the most common)
These are the least expensive
They are inert, meaning they do not interact with orbital tissues
They will not attach to orbital tissues, so they are more likely to move or become displaced within the orbit.
Integrated implants:
1. Pegging of the implant provides increased movement.
2. Larger implants can be used.
3. The muscles can be directly sewn to the implant.
For more information on enucleation you can go to a medical library, or click and order a copy of our comprehensive review of:
“Enucleation” by Moshfeghi DM, Moshfeghi AA, Finger PT. Survey of Ophthalmology 2000:44:277-301.
After seed implantation, an x-ray is used to document radioactive seed locations and allow for in vivo dosimetry.
By Paul T. Finger, MD
Dr. Finger has been using the Brachytherapy Boost Technique (BBT) for over 25 years. It is a multidisciplinary approach that can spare patients from exenteration surgery (removal of the eye and all the orbital contents).
During the BBT procedure, instead of removing the eye lids and orbital tissues, the bulk of the orbital tumor is removed and radioactive seeds or HDR catheters are temporarily placed in the tumor-bed. With this method, the area of tumor infiltration is irradiated more than the rest of the remaining ocular and/or orbital structures. An overlay of a reduced amount of external beam radiation therapy is typically given to the entire orbit or targeted zone.
Dr. Finger considers the brachytherapy boost technique in the following clinical situations
1. When the standard external beam radiotherapy would require using a dose so high that it would result in a blind and painful eye (e.g. orbital melanoma, squamous and basal cell carcinoma, adenoid cystic carcinoma).
Catheters (upper right) for radioactive seed implantation are placed at the time of surgery.
2. When exenteration of the orbit is the only option, but offers historically poor local control rates (e.g. adenoid cystic carcinoma).
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.