New Radiation Instructions for Eye Plaque Patients 2018
Based on published guidelines from United States Nuclear Regulatory Commission (NRC), The New York Eye Cancer Center and its affiliate New York Eye and Ear Infirmary of Mt. Sinai have agreed that patients undergoing low energy (iodine-125 or palladium-103) eye plaque radiation therapy for intraocular melanoma are allowed to proceed with their lives as usual.
Before this change, eye plaque patients were required to almost quarantine themselves. They had to remain at home, maintain a distance of 6-feet from others, and no pregnant women or children were allowed to visit.
With the new changes, patients can use public transportation. We ended most of the radiation exposure precautions and restrictions (i.e. you may go to the park, restaurants, grocery stores…etc.). However, it is recommended that patients stay at home as much as possible and that they do not engage in activities that could dislodge the implant and/or seeds. As before, the patient’s body fluids, clothing, and utensils ARE NOT radioactive and can be handled by others safely. We ask that the patient sleep alone and in a separate room away from anyone under the age of eighteen.
Dr. Finger says it’s about time: “With the radiation implants I use, eye cancer patients typically receive only a small fraction of the radiation given to patients undergoing implant radiation for other cancers, where patients are sent home on the day of implant.”
Though a few rules remain, they new radiation instructions are not nearly as strict. Free at last, patients can feel the sunlight, do their own shopping, and enjoy the company of their loved ones.
Byline: Published in The American Journal of Ophthalmology, 2019;198:45-53
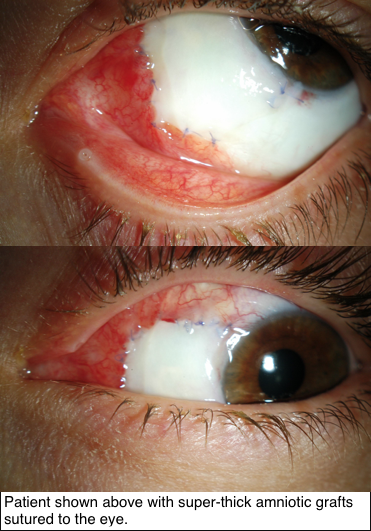
Since 1940, a single, thin layer of amniotic membrane graft (AMG) has often been used for repairing the cornea and conjunctiva. However, Dr. Finger says:
“our research shows that super-thick AMG (ST-AMG), up to ten times thicker than the prior AMG, is more effective for reconstruction of the eye’s surface.”
Research supported by The Eye Cancer Foundation has proved greater efficacy of this new technique in recreating the outer surface of the eye and inner surface of the eyelids. As published in the American Journal of Ophthalmology on November 2018, tumors of the conjunctiva and eyelids were surgically removed, then amniotic membranes from donor human placentas were sewn into the defects to recreate a normal ocular and inner eyelid surface.
Thus, amnion can provide a foundational platform for new cells to grow and flourish. In this case series, super thick amniotic membrane grafts (AMGs) were found to facilitate the healing of wounds.
How exactly does graft thickness affect the success of treatment? Well, the greater thickness means it is more easily sewn into the affected area, and
also helps the grafts to remain several weeks after placement. Thicker grafts are less likely to tear, rupture, or dissolve during the postoperative period. Most importantly, following treatment with ST-AMG, every single patient retained their sight and found their wounds successfully healed.
Super-thick amniotic membrane grafts have proven benefits to their thinner counterpart, and perhaps its versatility hints at potential for greater medical applications in the near future.
To keep up-to-date on the latest in Eye Cancer News, bookmark our website or follow us on facebook!
International Society in Ocular Oncology and The Eye Cancer Foundation will sponsor the Second Eye Cancer Working Day on the first day of the ISOO meeting, Friday, March 24, at the International Convention Centre in Sydney, Australia, at the Cookle Bay Room 1.
The Working Day provides an opportunity for eye cancer specialists from around the world to work together, face-to-face. Our goal is to help the subspecialty move forward into the mainstream of oncological care. This will require the creation of evidence-based medicine, educational programs, outreach to underserved areas, and multicenter quality assurance.
The 2017 Working Day will feature five separate committees focused on these ongoing initiatives. These include the topics of international medical evidence, retinoblastoma fellowships, quality assurance, surgical standards, and consensus guidelines.
MIR:Multicenter International Registries create statistically significant evidence. These registries will improve patient care and help us defend our methods of diagnosis and treatment.
FOR- RB: Retinoblastoma fellowship initiative to address the worldwide RB mortality.
DRO: Quality assurance through Doctors Reporting Outcomes. Eye cancer specialists cannot know how to improve, unless they know the outcomes of their work.
COAST: A Comprehensive, open-access, consensus-based surgery text.
RASER: A prospective ophthalmic Radiation Side Effects Registry
The FIRST Working Day was held at The Curie Institute in Paris immediately prior to the ISOO 2015, and it was a big success.
We are excited to have the SECOND Working Day integrated with the biannual ISOO meeting. If you’re an eye cancer specialist attending the conference, be sure to mark your calendars and arrive by Thursday night!
Second Eye Cancer Working Day Schedule
Time: 8:00am – 5:00pm
Room: Cookle Bay Room 1, International Convention Centre
Convenors: Paul T Finger, Santosh G Honavar
Time
Project
8:00am
Registration and Coffee
8:30am – 9:00am
8:30am – 8:45am
8:45am – 9:00am
Introduction
Paul T Finger
Santosh G Honavar
9:00am – 10:00am
Comprehensive Open Access Surgical Textbook (COAST)
Convenor: Santosh G Honavar
Faculty: Fairooz P Manjandavida, Carol Shields, Zeynel Karcioglu, Mandeep Sagoo, Paul T Finger, Santosh G Honavar, Hardeep Mudhar, Sonal S Chaugule
10:00am – 11:00am
Radiation Side Effect Registry (RASER)
Convenor: Wolfgang Sauerwein
Faculty: Wolfgang Sauerwein, Paul T Finger, Brenda Gallie
11:00am – 11:30am
Morning Tea
11:30am – 12:30pm
Fellowship Outreach Retinoblastoma (FOR-RB)
Convenor: Ashwin Mallipatna
Faculty: Ashwin Mallipatna, Helen Dimaras, Brenda Gallie, Guillermo Chantada, James Muecke, Nathalie Cassoux, Santosh Honavar, John Zhao, Yacoub Yousef, Peter Gabel
12:30pm – 1:30pm
Lunch
1:30pm – 2:30pm
Doctor Reported Outcomes (DRO)
Convenor: Tero Kivelä
Faculty: Tero Kivelä and faculty
2:30pm – 3:30pm
Multicenter International Registries (MIR)
Convenor: Bita Esmaeli
Faculty: Bita Esmaeli, Brenda Gallie, Martine Jager, Zeynel Karcioglu, Yulia Gavrylyuk, Paul T Finger
3:30pm- 4:00pm
Afternoon Tea
4:00pm – 5:00pm
Future Directions
Faculty: Santosh G Honavar, Martine Jager, Bita Esmaeli, Tero Kivelä, Ashwin Mallipatna, Wolfgang Sauerwein, Paul T Finger
**Please note that The ISOO Working Day workshop will be using live polling. Please ensure that you bring your mobile phone so that you can be an active part of the session.
1. Does your doctor spend as much time as you need to understand your condition and treatment options?
We all know the trend of medicine over the past several decades: doctors’ decisions are being pressured by outside forces and patients feel like they are being rushed along a conveyor belt of care.
At The New York Eye Cancer Center, Dr. Finger and his staff take the time to understand each patient’s needs, answer all questions, and ensure that critical details do not go overlooked.
This is why our practice does not directly participate in many major insurance plans – though we will assist patients seeking reimbursement. Our first priority is patient care that will not be sacrificed to government, hospital, or insurance company demands.
2. Which doctor will perform your surgery?
When you are referred to a specific doctor, you should see that doctor for the initial consultation and in the operating room. You should know what role other doctors, associates, fellows, or residents are taking in your procedures.
At The New York Eye Cancer Center, we think patients deserve to know who will be the primary surgeon for their operations. Your consultation and surgery will be performed by Dr. Finger, who has over 30 years experience treating eye cancers.
3. Who answers the office phone at night?
Find out who answers the phone after hours. Is it a voicemail or will you be sent to the emergency room after office hours?
At The New York Eye Cancer Center, our staff of doctors are trained to answer questions during the day, but care extends beyond office hours. We always have a live person answering our phone even after the office is closed. This ensures that emergencies will be handled by Dr. Finger or his staff at all times. In addition, non-emergency messages will be delivered to The New York Eye Cancer Center office every morning.
4. How familiar is your doctor with established and new treatments? What innovative treatments has your doctor developed?
Look up your doctor before you have your consultation. You can search their publications on http://pubmed.gov. You can also visit the doctor’s web site to evaluate their training.
Dr. Finger has written review articles on eye surgery, radiation, chemotherapy, and metastasis. He recently published the chapter on intraocular melanoma for DeVita’s Textbook of Medical Oncology, as well as the chapter covering all eye cancers in the UICC Manual of Clinical Ophthalmic Oncology.
Patients should also consider seeking a physician who actively contributes to medical advancements. This is not simply for the benefit of mankind, but demonstrates the doctor’s knowledge about his specialty’s state of the art.
Dr. Finger is a pioneer in his field, with 14 filed patents/trademarks and over 300 published medical journal articles and book chapters. Dr. Finger has developed many new medical devices, as well as innovative diagnostic and surgical techniques.
5. Does your doctor publish their results?
Clearly, patients do not want the most popular or the most sociable doctor – they want the doctor who will deliver the highest possible chance of preserving their life and their sight.
At The New York Eye Cancer Center, we have a long history of publishing our results in the medical literature. Recently, we were the first to place summaries of our published results online so that prospective patients can easily access them.
6. Will you be trapped in a system?
Many centers and insurance companies are run as self-contained medical systems. That means every aspect of your care is given within that system (consultations, surgery, radiation, chemotherapy, surveillance). While one-stop-shopping may be easy, it also can prevent you from seeing excellent physicians outside that network.
Dr. Finger is in private practice, so he is able to work with a network of independent service providers that stretch across New York City. Dr. Finger has the freedom to choose his preferred providers for each individual service. The result is his “dream team” of professionals who are each at the top of their field.
7. Are you treated with respect by all practice staff?
Cancer patients know the importance of hope and positivity in surviving this disease. Though appointments may unavoidably cause some anxiety, the doctor’s office should be a place to reinvigorate you in your battle. Patients deserve to be treated with care and respect not just by the doctor, but also by the front desk, billing, optometry, and other office staff. Patients should not be left waiting all day for a scheduled appointment. When emergencies are fit into the schedule, the staff should tell you and make you as comfortable as possible.
The New York Eye Cancer Center prides itself on the quality of each member of its staff. Every patient receives the highest level of care and respect, as you deserve.
Uveal melanoma (UM) is the most common primary adult intraocular cancer involving the vascular layer within the eye between the retina and the sclera. Researchers have long suspected that people with light pigmentation and blue eyes have an increased risk of developing this type of eye cancer. Previous studies show that about 12% of uveal melanoma manifest within family circles, often involving a variety of other cancers including skin cancer. The co-occurrence of skin cancer and UM within some families suggests a shared predisposition to both types of cancer.
But despite the suspicion that there are genetic risk factors involved in uveal melanoma, there has been little solid research establishing a firm link.
To study the possibility, researchers at the Perlmutter Cancer Center of the New York University School of Medicine selected 28 genetically based variations (SNPs) found within a given population of people. SNP variations have been shown to underly differences in susceptibility to diseases (such as sickle-cell anemia and cystic fibrosis) within different groups of people.
For the study, researchers conducted association analysis using 272 UM patients and 760 controls of European ancestry. Focusing on SNPs associated with skin cancer and related characteristics (including skin and eye pigmentation), they found five variants significantly associated with UM risk. In a nutshell, the study provides evidence that there is a link between light skin pigmentation (and blue eyes) and uveal melanoma:
“The identification of novel germline genetic loci involved in UM susceptibility in our study provides the first evidence of a link between the inherited genetics of pigmentation and UM risk. It has been established that lighter pigmentation and chronic sun exposure impact the development of choroid nevi, which occur in ~7% of the US population and are a known precursor for UM. Testing the associations in this study in the context of UM risk and the presence of ocular nevi will also be important in future analyses… Importantly, these genetic observations are also in clear alignment with previous epidemiological studies demonstrating that light eye color is indeed a UM risk factor.”
The association between skin cancer, uveal melanoma, and the emerging evidence of some genetic predisposition for the development of uveal melanoma underscores the importance of fair-skinned people protecting their eyes from sun exposure just like they do their skin. Since you can’t rub suntan lotion on your eyeballs, it’s important to wear sunglasses that provide 100% UV protection. Think of sunglasses as sunblock for your eyes. In fact, it’s a good idea for everybody to wear UV-cancelling sunglasses to protect their eyes from dangerous ultra-violet light rays.
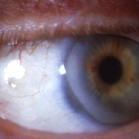
External photograph shows the pigmented tumor “melanoma” in the conjunctiva.
By Paul T. Finger, MD
Current treatments for conjunctival cancer has included surgical removal, removal with subsequent cryo-(freezing)-therapy, radiation therapy, and chemotherapy eye-drops. While most treatments have focused on avoiding large surgeries which may (in very severe cases) be associated with vision loss or loss of the eye, these decisions have been made with the knowledge that conjunctival cancers are serious. They can invade into the orbit (tissues around the eye), the sinuses, and the brain. Conjunctival melanomas and squamous carcinomas can also spread (metastasize) to other parts of the body. Because of high recurrence rates after standard treatments and the desire to avoid surgery, recent investigations have focused on topical chemotherapy “eye-drops.”
For a more detailed explanation of the risks and potential benefits of topical chemotherapy for conjunctival cancers, the editor suggests you obtain and read the referenced manuscripts.
After 28 days of topical MMC chemotherapy the tumor regressed.
Conjunctival Melanoma and PAM with Atypia
In 1993, Dr. Finger was the first to use mitomycin chemotherapy eye-drops to treat conjunctival melanoma and primary acquired melanosis. Since that time, it has become commonly and widely used throughout the world. It is currently used to reduce the tumor prior to surgical removal and with surgery for cases where there is too much normal tissue involved (too much for surgery and/or freezing (cryotherapy).
In addition, Dr. Finger discovered that topical interferon chemotherapy (Intron A) eye drops can be used to treat superficial conjunctival melanoma.
Topical chemotherapy eye drops can be used as primary treatment, as well as an addition to surgery and cryotherapy. Since almost all conjunctival tumors have different sizes, shapes and locations, your eye cancer specialist should know when and if you are a candidate for topical chemotherapy.
Squamous Conjunctival Neoplasia
Chemotherapy eye-drops have also been investigated as an alternative treatment of squamous conjunctival – corneal neoplasia. For more information consider reading the following manuscripts. Squamous Conjunctival Neoplasia
References
Finger PT, Milner MS, McCormick SA. Topical chemotherapy for conjunctival melanoma. British Journal of Ophthalmology 77:751-3, 1993
Frucht-Pery J, Pe’er J. Use of mitomycin C in the treatment of conjunctival primary acquired melanosis with atypia. The Archives of Ophthalmology 1996;114:1261-1264.
Finger PT, Czechonska G, Liarikos S. Topical mitomycin C chemotherapy for conjunctival melanoma and PAM with atypia British Journal of Ophthalmology 82:476-9, 1998
Finger PT, Sedeek RW, Chin KJ. Topical interferon alfa in the treatment of conjunctival melanoma and primary acquired melanosis complex. Am J Ophthalmol. 2008 Jan;145(1):124-129.
Danapoulos ED, Danpoulous IE, Liarikos SB et al. Effects of urea treatment in malignancies of the conjunctiva and cornea. Ophthalmologica 178:198-203, 1979
De Keizer RJW, de Wolff-Rouendaal, van Delft JL, et al. Topical application of 5-FU in premalignant lesions of the cornea, conjunctiva, and eye lid. Doc Ophthalmol 64:31-42, 1986.
Frucht-Pery J, Rozenman Y. Mitomycin C treatment for conjunctival -corneal intraepithelial neoplasia: A multicenter experience. Ophthalmology 104:2085-2093, 1997
Wilson MW, Hungerford JL, George SM, Madreperla SA. Topical mitomycin C for the treatment of conjunctival and corneal epithelial neoplasia. American Journal of Ophthalmology 124:303-311, 1997
The authors examined if the American Joint Committee on Cancer (AJCC) staging system for ocular adnexal lymphoma (OAL) could be used to predict local control and systemic disease. A multicenter, consecutive case series of patients with biopsy-proven conjunctival, orbit, eyelid, or lacrimal gland/sac lymphoma was performed.
Results
They found that extranodal marginal zone B-cell lymphoma of mucosa-associated lymphoid tissue was the most common and AJCC clinical stages were cT1NOMO (21.7%), cT2NOMO (44.6%), cT3N0M0 (5%), and cT4NOMO (2.4%).
Treatment was able to control the local tumor in 75% of patients.
Of the 19 local recurrences, 74% (most) were found after non-radiation based treatments.
The lower-risk “smaller tumor” AJCC T1 and T2 groups without lymph node involvement or metastatic disease had longer disease-free survival than the higher-risk AJCC T1, T2 with nodal involvement or metastatic disease, AJCC T3, and T4 as well as Ann Arbor II, III, and IV.
Conclusions
Regardless of stage, recurrence and disease-free survival were more closely related to having had radiation treatment and histopathology rather than site specific factors, such as tumor size or location around or behind the eye.
Q: Can the laser be used to treat an eye melanoma?
A: Most studies have shown that the laser treatment just burns the surface of the melanoma. This can leave live cancer cells under the tumor’s laser scarred surface and in the wall of the eye. It may be just a matter of time before the cancer will grow again. If the cancer is not killed or removed, there is a chance that it might spread to the rest of your body.
Due to the high incidence of failure using Transpupillary Thermotherapy (TTT) laser alone, it is rarely used without additional plaque radiation for choroidal melanoma. However, intraocular hemorrhages are common, and in rare cases the wall of eye (sclera) can be weakened allowing tumor growth into the tissues behind the eye.
In contrast, TTT laser is commonly successful in treatment of small retinoblastomas.
Q: Can you surgically remove the tumor and leave my eye?
A: During this type of surgery the eye must be opened. Though not a proven risk for metastasis, eye wall resection allows tumor cells to float out of the eye and into the orbit (spaces around the eye).
With lamellar (split thickness) eye wall resection, the wall of the eye (sclera) is sewn back in place. The COMS study showed that up to 50% of choroidal melanomas had invaded the wall of the eye. Therefore, with lamellar eye wall resection, the entire tumor is not always removed or treated. In order to prevent recurrence, eye cancer specialists are currently adding plaque therapy to treat the eye wall. Lastly, depending on the skill of the operating surgeon, many eyes do not tolerate eye wall resection. These eyes suffer sight limiting retinal detachment, cataract, and intraocular hemorrhage.
Q: How long will I have to be a patient?
A: For the rest of your life. You must be followed by an eye-care specialist and may need a medical oncologist. You may want to consider this when choosing your doctors and their location.
Patients who receive plaque radiotherapy are typically seen by their eye care specialist every 3 to 4 months. Patients may undergo twice-yearly blood tests, radiographic imaging studies and physical examinations. Patients being treated for radiation retinopathy and/or optic neuropathy may have to be seen every 4-6 weeks.
Copies of your laboratory evaluations should be forwarded to your eye cancer specialist’s office, so they can be double-checked for metastatic disease. In the United States, the law requires that you must request this in writing from your family doctor, internist, or oncologist.
Q: How will having a choroidal melanoma affect my life?
A: Almost all patients who have been determined to have an ocular tumor (e.g. choroidal melanoma) are treated and then return to their normal activities.
The time between the diagnosis and the completion of treatment can be very stressful. Rely on your doctors and family for help. After you are treated they should encourage you to get back to your normal activities. Just remember to be periodically monitored by your eye care specialists and general medical doctors.
Q: What are the standard treatment options?
A: Standard treatments for choroidal melanoma are enucleation and radiation.
Enucleation means removal of the eye. In most cases, it is the only form of treatment that allows your doctor to completely remove the tumor from your body. Unfortunately, patients also lose their vision and the cosmetic use of the eye. With time, almost all patients are able to do all the things they used to before losing their eye. Since the COMS study found no difference in survival between enucleation and plaque radiation therapy (for medium-sized melanomas), few doctors will recommend enucleation if “eye-sparing” radiation therapy is possible.
The most common alternative to removal of the eye is radiation therapy, and the most commonly used radiation technique for intraocular melanoma is eye-plaque radiation therapy.
Plaque technique involves placing a dish-shaped plaque-device (about 1 to 2 centimeters in diameter) on the outer surface of the eye, under the tumor. The plaque is implanted behind the eye, left in place for up to 5-7 days, and then removed. During treatment patients are likely to notice no more than occasional discomfort.
The effects of radiation on the tumor are typically measured 3 to 4 months after treatment. Eventually, eye melanomas shrink to about 40% of their pretreatment size. Though they rarely disappear, these tumors are considered to be dead. In most studies, irradiated tumors will regrow (within the eye) in less than 8% of cases. Local control means the tumor was killed. Ask your doctor about their rates of local control after treatment and for how long those patients were followed (typically reported at 5 and 10 years after treatment). You can see The New York Eye Cancer Center’s local control rates on our outcomes page.
Note about radiation: More than 95% of patients have no problems associated with plaque surgery. As with any ocular surgery, there can be secondary retinal detachments, hemorrhages, or infections. There are also the regular risks related to hemorrhage, infection or reaction to anesthesia. Most plaque patients do not develop these problems.
Q: What research is being done for ocular melanoma?
A: Around the world, researchers are working on new methods of diagnosis and treatment for choroidal melanoma, retinoblastoma, and other ocular tumors. One only has to do a PubMed search to find thousands of published articles.
It is important to point out two major research initiatives:
The first multi-center, multinational prospective randomized clinical study carried out for an eye cancer was called The Collaborative Ocular Melanoma Study (COMS). These types of studies offer the best evidence-based statistically significant information currently available. The National Eye Institute (NEI) and the National Institute of Health (NIH) supported the COMS.
The COMS had three studies:
The Small Choroidal Melanoma Study confirmed that orange pigmentation, leakage of fluid, and thickness are all correlated to tumor growth and metastatic potential. This study also found that there exists a risk of metastatic melanoma from small choroidal melanomas.
The Medium-Sized Choroidal Melanoma Study determined that plaque radiation was equal to removal of the eye for the prevention of metastatic choroidal melanoma.
The Large-Sized Choroidal Melanoma Study determined that 2000 cGy of external radiation prior to enucleation does not prevent the spread of choroidal melanoma.
The second major collaborative step forward was when The American Joint Committee on Cancer joined with the International Union Against Cancer to develop a Tumor-Node-Metastasis (TNM) grading system for most eye cancers. It is our hope that this common language will enable centers (around the world) to compare their results.
Q: What usually happens to a patient’s vision after treatment?
A: Enucleation
After enucleation (removal of the eye) there is no vision from that eye. The patient is considered monocular and sees from the remaining eye. Most patients see well from their remaining eye and live normal lives. Loss of one eye does affect depth perception, but with time, most patients are able to adjust. Consider that part of depth perception comes from the relative size of objects (distant objects appear smaller).
A: Plaque Radiation Therapy
Prior to treatment for radiation-related damage to the retina and optic nerve, post-plaque radiation therapy for choroidal melanoma caused vision loss in half of patients within 5 years. However, with the use of laser treatment and/or intraocular anti-VEGF drug therapy, the vision destroying radiation retinopathy can be suppressed. Anti-VEGF suppression of radiation retinopathy and optic neuropathy has preserved patient vision for years. Further, the natural eye looks and moves better than an ocular prosthesis.
Disadvantages of plaque versus enucleation include that you must see an ophthalmologist every 3 to 4 months after treatment for dilated ophthalmoscopy and ultrasound measurements of your tumor. This is because patients who have their eye irradiated (plaque or proton) develop radiation complications within the eye, and there is a small chance that the tumor might regrow.
The patient’s chance for functional vision after radiation is related to how close the tumor is to the functional center of the retina (macula), the type of radiation, and the dose delivered to normal ocular structures. The American Brachytherapy Society Consensus Guidelines suggest that all centers perform pre-operative comparisons of plaque types for dose to normal eye structures.
Q: Will the tumor spread to other parts of my body?
A: Less than 4% of patients are found to have metastatic melanoma at the time of diagnosis. But with time after treatment, a much larger percentage are found to develop metastasis. This difference is thought to be due to undetectable microscopic melanoma cells present at the time of treatment. It is not helpful to dwell on percentages, but your doctor should be able to give your approximate chance of developing metastasis based on your tumor’s size and location.
About Enucleation Surgery
Q: If I must lose my eye, will it hurt?
A: The eye is surrounded by bones; therefore, it is much easier to tolerate removal of an eye as compared to loss of a lung or kidney.
Almost all enucleation surgery can be performed as an outpatient. Older patients and those with significant systemic medical problems may have to stay in the hospital after surgery.
Since this surgery is usually performed under general anesthesia, the patient does not feel or see anything during surgery. Long-acting local anesthesia (6 hours) can be given during surgery, allowing for the least amount of pain possible (when you wake up in the recovery room). Most patients who have their eye removed have a mild headache for 24-36 hours after surgery.
Q: What is enucleation?
A: Enucleation is removal of the eye. It is the form of treatment that allows your eye cancer specialist to remove the tumor from your body. Unfortunately, patients also lose all the vision and the cosmetic use of the eye. With time, almost all patients are able to do most all the things they used to do before their eye was removed.
Q: What might I look like after enucleation?
A: This is a patient who has completed cosmetic rehabilitation after enucleation surgery. Notice that he looks normal, but the prosthetic eye does not move as well as a normal eye.
Q: When will I get a prosthetic eye?
A: Patients can usually have a temporary prosthesis (that looks like an eye) within 10 days of enucleation surgery. Besides the swelling and the “black-eye,” you will look fairly normal. After a final prosthetic fitting, 90% of patients are happy with the way they look, and 80% say others can’t even tell they are monocular.
Read the book A Singular View, by Frank Brady. It will help in your transition. This book was written by an airplane pilot who lost one eye. We suggest that you wear unbreakable polycarbonate glasses to protect your good eye.
Q: Why are very large-sized tumors treated by removal of the eye?
A: This is because the amount of radiation required to kill a large tumor that fills most of the eye is just too much for the eye to stand. Within months to years, many patients who are treated with radiation for very large ocular melanomas lose vision, develop glaucoma, or have their eye removed anyway. It is important that the eye cancer specialist inform each patient regarding their approximate chance of developing radiation associated complications. Despite these risks, more and more patients with large intraocular tumors are treated with eye and vision-sparing radiation therapy.
Frequently Asked Questions After Enucleation Surgery
Q: How long will I have to be a patient?
A: For the rest of your life. You must be followed by an eye-care specialist and may need a medical oncologist. You may want to take this into account in choosing your doctors and their location.
An eye care specialist examines patients who are enucleated twice a year. In addition, patients should have blood tests, radiographic imaging studies, and physical examinations. Copies of your laboratory evaluations should be forwarded to your eye-cancer specialist’s office so they can be double-checked for metastatic disease. The law requires that you must request this in writing from your family doctor, internist, or oncologist.
Q: How often will I need to be checked after enucleation?
A: Dr. Finger recommends that you have an eye examination within 1 week, 1 month, and at least every 6 months after surgery. This is to monitor for inflammation or infection, and because there is an extremely small chance the tumor will regrow behind your prosthesis.
Dr. Finger recommends that you return for a complete ophthalmic oncology examination at least on a yearly basis. You should also have twice-yearly medical check-ups by your family doctor, internist, or medical oncologist.
Q: What sort of care will my eye need after I go home?
A: You will be advised to take topical antibiotic and steroid medications for one month. These medicines will help you heal more safely and quickly.
For the first week after surgery, you will tear a lot. These tears may contain a little blood. This is normal. Once a day, you should gently wash the outside of your eyelid with a warm, clean, soapy washcloth. Don’t let matter accumulate to form a crust on your eyelids.
Q: What will happen to my vision?
A: Enucleation means removal of the eye. It is a form of treatment that completely removes the primary tumor from the body, but the patient loses all vision and the cosmetic use of the eye. It takes some time to adjust to using one eye, but almost all patients learn to compensate within the first year after surgery.
Q: When can I get a prosthesis?
A: Dr. Finger can usually place a temporary prosthesis (that looks like an eye) within 10 days of enucleation surgery. Most patients are fitted with a permanent prosthesis 4 to 6 weeks later.
Q: When can I go back to normal activity?
A: Do not lift, strain, or rub your eye for at least 14 days after surgery.
Do not take aspirin or other blood thinners unless your internist says it is required. The orbit should heal quickly, and you should be able to return to school or work within 2 to 6 weeks after surgery.
Q: When can I wash my hair and face?
A: You should gently clean your lids each day. You may use a clean wash cloth and baby shampoo. You should not rub your eyelids or run the shower at your operated eye for at least 10 days after surgery.
How do I choose an Eye Cancer Specialist?
Q: How do I pick a doctor?
A: You should pick a doctor who has experience caring for eye cancer patients and with whom you are comfortable. You should be able to ask questions about your case and feel comfortable that your treatment decisions are not only based on available science, but also take into account your personal situation and medical problems. Since you may need to see your doctors for many years, consider that it is easier to be treated and followed with a doctor in your area.
Consider the following:
You should be guaranteed to see the doctor with whom you are making the appointment (not a substitute doctor). Ask when making your appointment.
Make sure that your surgeries will be performed by the doctor you want. Ask the doctor who will be performing your surgery when signing your consent form.
You should be able to ask questions about your case and treatment decisions.
Ask how easy it is to speak with your doctor before and after surgery.
Ask what happens when there is an emergency during nights and weekends.
Make sure your doctor has the expertise to manage any eye and/or systemic problems you may have in the future.
Q: How long will I have to be a patient?
A: For the rest of your life. You must be followed by an eye cancer specialist and may need a medical oncologist. You may want to take this into account when choosing your doctors and their location. Patients who receive plaque radiotherapy are typically seen every 3-4 months. Patients who are enucleated are usually seen twice a year. Many eyelid and orbital tumor patients are advised to follow up with their eye cancer specialist, at least, on a yearly basis.
In any case, your eye care specialist should check to make sure that you have regularly scheduled medical workups, including an evaluation for metastatic disease (as necessary). Copies of your laboratory evaluations should be forwarded to your eye-cancer specialist’s office so that they can be double-checked. The law requires that you must request this in writing from your family doctor, internist, or oncologist.
Enucleation: About Ocular Prosthesis Care
Ocular Prosthesis
Q: How do I remove my prosthesis?
1) First, wash your hands.
2) Then you should place a towel over your lap or sink to act as a net for the prosthesis if it slips out of your hand. Should it fall it could scratch, break, or get lost.
Manual Technique
3) Place one finger on the temporal (towards the ear) aspect of the lower lid on top of the cheek bone.
4) Look up.
5) Cup your other hand under your eye (to catch the prosthesis).
6) Gently press your finger in and pull the eyelid skin towards your ear (on that side).
7) The edge of your prosthesis will likely be emerging at the edge of the lower eyelid, or (less likely) it has fallen into your cupped hand.
8) If the prosthesis is just barely out, you can use a finger on your other hand to rotate it out of the socket.
9) Don’t be surprised if some discharge comes along with the prosthesis.
Suction Technique
1) Hard contact lens suction devices are commercially available in drug stores and vision centers.
2) These devices can be squeezed to create a vacuum that attaches the device to the front of the prosthesis.
3) Once attached, the patient can lift the bottom portion of the prosthesis out from beneath the lower lid, then slide the superior portion down towards the cheek.
Once the Prosthesis Is Out
1) Commercially available sterile saline solution should be used to clean your eye socket.
2) Now you can consider cleaning the prosthesis.
Q: How do I clean my prosthesis?
1) Place the prosthetic eye into a container that can be filled with liquid as to cover the prosthesis.
2) Full or half strength hydrogen peroxide solution can be used to soak the prosthesis for 10 to 15 minutes. After soaking, remove the prosthesis from the container and rinse it with sterile saline solution.
3) Prosthesis cleaning is typically performed once or twice a week (as instructed by your eye care professionals).
4) Continuous and consistent periodic cleaning of the prosthesis will increase your comfort, decrease secretions, prevent secondary conjunctivitis and extend the life of your ocular prosthesis.
Q: How often do I need to have my prosthesis professionally cleaned or replaced?
1) You should return to your ocularist for professional cleaning and polishing 2 times each year.
2) Most patients get a new prosthesis every 3 to 5 years because even with excellent maintenance, the tissues around the prosthesis can change and the artificial eye can become scratched.
Warning!!!
If you notice excessive discharge, swelling or irritation, you should call your eye care professional immediately.
Related Links
For the more medically minded, you can go to a medical library, or click and order a copy of our comprehensive review of:
A: No! Once the radiation plaque is removed, all the radioactivity is gone. There will be no radiation left in your body, your clothing, your glasses, or any of your personal belongings. However, the effects of the radiation delivered to your tumor and eye will continue to be observed for months and years after treatment.
Q: How often will I need to be checked after plaque treatment?
A: We recommend that you be examined every 3-4 months after plaque radiation. This is because there is a small chance the tumor will regrow or that your eye may develop radiation-related problems (that may require treatment).
In addition to seeing your local eye care specialist, we recommend that you return for a complete ophthalmic oncology examination (at least) on a yearly basis.
You should also have twice-yearly medical check-ups by your family doctor, internist, or medical oncologist. Dr. Finger recommends that you have a medical checkup at least two times a year. This should include a physical examination and radiographic imaging of the abdomen.
Q: How quickly will my tumor go away after plaque radiation?
A: Tumors are usually measured to shrink after 3 months. We don’t measure a tumor before three months, because they can swell and become temporarily larger after radiation, unnecessarily frightening patients. Since the goal of radiation therapy is to prevent the tumor from growing, don’t be concerned if your tumor shrinks slowly. Most tumors eventually shrink to about 40% of their original size and rarely disappear. A residual lump of dark, shrunken tumor typically persists for years after treatment.
Q: How soon can I return to normal activities?
A: The eye should heal quickly. You should not lift any objects greater than 10 pounds or rub your eye for at least two weeks after surgery. Then you can return to normal activity. Patients usually return to school or work within 2-4 weeks after completion of treatment. If the tumor has caused a retinal detachment, it may take longer for you to return to normal activities.
Q: What after-care will my eye need after I go home?
A: After ophthalmic plaque radiation therapy, the patient is usually requested to take eye-drops daily for about a month. These drops contain antibiotics, steroids, and medicines to relax your eye. These drops help your eye heal more safely and quickly. For the first week after surgery, you will tear and the tears may contain a little blood. This is normal. You should gently wash the outside of your eyelid with a warm, clean, soapy wash cloth. Don’t let matter accumulate to form crust on your eyelids.
Q: What are the differences between Protons versus Plaques?
A: Proton Beam Radiotherapy is a form of external beam irradiation. It involves directing radiation through the front of the eye, lids, and orbit in order to reach the intraocular tumor. Eyelash loss, eyelid excoriation, corneal neovascularization and ulceration, dry eye, neovascular glaucoma, and cataract have been reported to be more common after proton beam radiation therapy.
Proton beam radiation therapy typically requires surgical clips to be sewn onto the eye (around the tumor) this helps the radiation therapist to direct the beam into the eye. Eye movements are monitored on a video screen because if the eye moves, the beam moves away from the tumor. If the eye is detected to move, the radiation technologist will temporarily turn off the beam until the eye is repositioned. In contrast, radiation eye plaques are sewn onto the eye as to cover the base of the intraocular tumor. So when the eye moves, so does the plaque. With eye plaque, eye movement is not thought to appreciably affect the distribution of radiation within the eye.
Both proton beam and Fingers’ slotted plaques can be used to treat certain tumors that are near, touch or even surround the optic nerve.
Eye-Plaque Radiotherapy typically involves attaching a dish-shaped radiation source beneath the tumor and leaving it there for 5-7 days. With proton beam, once the marking clips are surgically placed, the patient visits the radiation center for 3-5 treatments. The marker-clips are not typically removed.
Compared with Proton-Beam, the front of the eye usually receives much less radiation with plaque radiation therapy, but parts of the retina may receive more. This is why anterior “front of the eye” complications are much less commonly reported after low-energy ophthalmic plaque radiation therapy.
Q: What is a radioactive eye-plaque?
A: A radioactive eye-plaque is a device that can be used to deliver a high-dose of radiation to an intraocular tumor.
This is because when an eye-plaque contains radioactive iodine-125 or palladium-103 seeds, the gold of the plaque blocks more than 99% of radiation. Therefore, when the plaque is sewn to the outside of your eye (underneath the tumor), the radiation is directed into the eye. For an average-sized tumor, less than 10% of the radiation makes it out of the other side of the eye.
Plaques come in various sizes (diameters between 10 to 22 mm). A plaque will be chosen to cover your entire tumor plus at least a 2-millimeter “safety margin”. The extra area is included to make sure the entire tumor is within the targeted area. The plaque is implanted utilizing several standard techniques (transillumination, ophthalmoscopy and ultrasound). Intraoperative ultrasound imaging and light-assisted plaque localization are techniques developed to make plaque-placement more accurate (see innovations).
Radiation treatment is continuous and will typically take up to 7 days. At the end of treatment, your tumor will have been given all the necessary radiation. Once your plaque is removed, there will be no radioactivity left in your body.
Radioactive plaques come in various sizes with suture eyelets so that it can be temporarily attached to the wall of the eye for treatment.
Q: What is plaque radiation therapy?
A: Radioactive plaque therapy is a form of treatment, which allows the eye-cancer specialist to destroy your tumor without removing the eye. Unfortunately, the radiation can also affect the normal parts of your eye and harm your vision. Your ophthalmic and radiation oncologists will work together to try to increase the effectiveness of radiation (to kill your cancer), while decreasing the chance that radiation will harm the normal parts of your eye.
Q: What is proton beam radiation therapy?
A: Protons are charged nuclear particles that can be sent into the eye. These particles travel through and are somewhat absorbed by tissues on the way to your intraocular tumor. The targeted zone (the tumor and surrounding 2-3 mm) gets most of the radiation. The proton radiation field is in the shape of a tube, with little side-scatter or dose posterior to the eye. Like plaque radiotherapy, the amount of radiation to the normal parts of the eye depends of the size and location of the tumor.
Q: What radiation precautions must be taken?
A: While the radiation-plaque is sewn onto your eye, certain precautions must be observed. These rules will ensure that visitors and patients in surrounding areas do not receive radiation exposure in excess of the Nuclear Regulatory Commission (NRC) regulations. A list of rules are given to you before you go home with the plaque in place and can be disregarded after you have the radiation-plaque removed.
Q: What will happen to my vision?
A: Radiation may cause eventual blurring, dimming, or rarely a total loss of vision (in the eye with the tumor). The amount of vision loss depends on what your vision was before treatment, how close the tumor is to the center of your retina (the fovea), and how sensitive your tissues are to radiation. Most plaque-irradiated eyes maintain some central vision, and almost all retain peripheral vision. Plaque radiation should not affect the vision in the other eye.
Q: Why does the plaque stay in place for up to 7 days?
A: Plaque radiation therapy is delivered over to a dose known to destroy the cancer, and at a dose rate that will be tolerated by the eye. The rate at which the radiation is delivered is affected by both the radiation source and the size of the tumor.
In consultation with the radiation oncologists, eye plaques are individually designed and constructed for each patient. Specialized computer programs are used to calculate the total dosage and speed of radiation. The precise distribution of radiation throughout the eye is calculated and used to determine the risks of secondary radiation complications.
Q: Will my hair fall out from radiation?
A: It is normal for patients to have fears about radiation.
The type of radiation used in most eye plaque therapy should not cause hair loss, nausea, brain damage, or affect your other eye.
Other forms of radiation therapy can cause hair loss within the field of irradiation. For example, proton beam radiation therapy is associated with eyelash loss. External beam therapy can also cause hair loss where it enters and exits the head.
Q: Should I Get a Second Opinion?
A: Second opinions are great when all your doctors say the same thing. Unfortunately, differing opinions can make things even more confusing. Remember to ask the doctor:
What are the standard treatment options for my tumor?
If the proposed treatment is “new” or investigational? If so, how many patients have been treated? How long have they been followed for recurrent disease?
What have your doctor’s results been for tumor control and vision retention?
Is the proposed treatment FDA or CE approved?
Who will be the operating surgeon? In the case of plaque therapy; who will put it in and who will take it out?
Does your center compare radiation plaque types (before surgery) to determine which one would be best for my tumor?
Does your center keep plaque patients in the hospital or send them home during treatment and why?
Does your eye cancer specialist and center personally follow treated patients for recurrence and metastatic disease?
How soon will you ask me to return after surgery?
What tests do you perform (over time) to monitor my body for metastatic disease?
What does your eye cancer specialist do if I am found to have metastatic disease?
What About Retinoblastoma?
Q: Until what age can a child develop another retinoblastoma?
A: Most retinoblastomas are diagnosed before the age of 3. Most eye cancer specialists agree that a child with retinoblastoma is not likely to develop a new tumor after 7 years of age.
Q: What are the most common symptoms of retinoblastoma?
A: Most children are found to have a white pupil “leukocoria,” or a deviated eye “strabismus,” or secondary painful glaucoma. In less developed countries patient more commonly present with orbital or optic nerve extension or metastasis.
Q: What other eye diseases can cause leukocoria “white pupil?”
A: Other than retinoblastoma, cataract, Coat’s disease, persistent hyperplastic primary vitreous, and retinopathy of prematurity can cause the appearance of a white pupil.
Q: Who gets retinoblastoma?
A: There are typically 325 of new cases of retinoblastoma diagnosed each year in North America. Ten thousand cases are estimated to occur throughout the world. Retinoblastoma occurs equally in boys and girls, different ethnic groups, and in either eye.
Retinoblastoma is a genetic cancer. Therefore, 10% of patients will have a family history of retinoblastoma, and 25% will affect both eyes. Forty percent of patients have the retinoblastoma gene throughout their body. The abnormal gene is 13q14.2, that is chromosome 13, long arm (q), band 14.2. Though it is the most common primary intraocular cancer in children, intraocular leukemia is more common.
Von Hippel-Lindau (VHL) disease is an autosomal dominantly inherited multisystem cancer syndrome with a predilection for the central nervous system (CNS) and the retina. Retinal capillary “Vvon Hippel” hemangioma is one of the most common and often the earliest manifestations of VHL disease and, therefore, ophthalmologists are frequently involved in the care of patients with this disease. The incidence of VHL disease is approximately one in 40,000 live births and it is estimated that there are approximately 7,000 patients with VHL disease in the United States.
Symptoms
Ophthalmic Findings:
The main ophthalmic finding in VHL is retinal capillary hemangioma, which is a benign hamartoma. The anterior segment can be secondarily involved due to complications such as neovascular glaucoma and cataract formation. A large cohort study found only 2% of eyes had neovascularization of the iris. If a patient has a solitary retinal capillary hemangioma, they do not necessarily have VHL disease. However, they should undergo genetic testing.
Diagnosis
Retinal capillary hemangiomas are usually orange red, circumscribed, round, vascular tumors supplied by a pair of dilated and tortuous feeder vessels. They are most commonly located in the temporal peripheral retina. Juxtapapillary retinal capillary hemangiomas are less common, representing about 11% to 15% of cases, and their appearance can vary depending on whether the lesion is endophytic (grow from the retina into the vitreous gel of the eye), exophytic (grow beneath the retina), or sessile (flat).
Retinal capillary hemangioma usually manifests as a solitary tumor, but approximately one-third of patients have multiple retinal hemangiomas, and up to half of patients have bilateral involvement.
Secondary effects (from the retinal angioma) leading to visual loss, such as intraretinal and subretinal exudation, are often limited to the vicinity of the hemangioma but can be remote, often producing a macular star of exudates. Glial proliferation can lead to tractional retinal detachment and macular pucker. Retinal or vitreal hemorrhages are rarely observed, occurring in fewer than 3% of cases.
Frequency and Patient Related Findings:
The frequency of occurrence of retinal capillary hemangiomas in VHL disease has been
reported to vary from 49% to 85%. The mean age at diagnosis of retinal capillary hemangioma in VHL disease is approximately 25 years, and most patients present between the ages of 10 and 40 years. The probability of developing a retinal capillary hemangiomas increases progressively with age. Recent publications indicate that the hemangioma is usually manifested by age 30, and the prevalence rate is stable thereafter. Therefore adults with a normal retina at age 30 years may have a low risk of developing a retinal capillary hemangioma during the reminder of their lives. The natural course of retinal capillary hemangiomas is variable (progression, stability or spontaneous regression). Small lesions may remain stable for years or may show evidence of gliosis without leakage, but some have been documented to enlarge. Most hemangiomas, however, tend to enlarge progressively and lead to retinal changes. In late stages they may cause massive exudation and retinal detachment, uveitis (inflammation), glaucoma and phthisis (shrinking of the eye). Classification systems to aid in staging the clinical progression have been developed.
Other Tumors That May Look Like Von Hippel Angiomas:
The fundus findings of retinal capillary hemangioma are usually typical, and diagnosis can be made based on ophthalmoscopic examination. The diagnosis might be confused with retinal macroaneurysm or adult Coats disease when severe exudation exists.
Treatments
For treatment of Von Hippel retinal angiomas, see Conditions (Von Hippel Angioma) However, in ths section we will discuss the diagnosis of systemic disease and genetics:
The systemic manifestations of VHL are multiple and include CNS hemangiomas of the brain and spinal cord, renal cell carcinomas, renal cysts, pheochromocytomas, pancreatic cysts, islet cell tumors, epididymal cystadenomas, endolymphatic sac tumors of the inner ear, and adnexal papillary cystadenomas of the broad ligament. After retinal capillary hemangioma, the most frequently affected organ systems are the CNS, kidneys and adrenal glands, many of them occurring years after the initial presentation with retinal capillary hemangiomas.
The diagnosis of VHL disease is based on three elements which include:
retinal capillary hemangioma or CNS hemangioma
visceral lesions
family history of similar lesions
Surveillance:
After diagnosis is made, screening protocols should be followed, including urinary catecholamines and ophthalmoscopy on an annual basis with MRI of the brain and spinal cord every 2 to 3 years, and yearly abdominal US with an additional abdominal CT scan every 2 to 3 years.
Genetic Testing:
VHL disease is an autosomal dominant disease whose gene is located on chromosome 3p 25-26. The gene functions as a tumor suppressor gene that promotes tumor formation when its function is lost. The normal protein product of the VHL gene forms a complex with other proteins that targets hypoxia inducible factors (HIFs) for degradation. Mutations in the VHL gene result in stabilization of the HIFs, which bind to specific enhancer elements in the VEGF gene and stimulate angiogenesis. With a near-complete penetrance of the disease and only rare instances of mosaicism, genetic testing has been proved helpful in early diagnosis and clinical screening for disease manifestations.
SUMMARY
VHL disease is an autosomal dominantly inherited multisystem cancer syndrome with a predilection for the central nervous system and the retina. Retinal capillary hemangioma is one of the most common and earliest manifestations of VHL disease. Fundus findings are usually typical, and diagnosis can be made based on ophthalmoscopic examination, but fluorescein angiography is an additional informative diagnostic tool. Various treatment modalities exist, although the mainstays of therapy are laser photocoagulation and cryotherapy. VHL disease, however, is associated with significant mortality secondary to either CNS hemangioma or renal cell carcinoma. Life expectancy of affected individuals can be improved by early detection, genetic testing and systemic treatment. Treatment of this syndrome requires cooperation of physicians from multiple specialists, including those to treat the central nervous system and kidney tumors.
References
Annesly WJ, Leonard BC, Shields JA, Tasman WS. Fifteen year review of treated cases of retinal angiomatosis. Trans Am Acad Ophthalmol Otolaryngol. 1977;83:446-453.
Choyke PL, Glenn GM, Walther et al. The natural history of renal lesions in von Hippel- Lindau disease: a serial CT study in 28 patients. Am J Roentgenol. 1992;159:1229-1234.
Dahr SS, Cusick M, Roudriguez-Coleman H, et al. Intravitreal anti-vascular endothelial growth factor therapy with pegaptanib for advanced von Hippel-Lindau disease of the retina. Retina. 2007;27:150-158.
Harris AL. von Hippel-Lindau syndrome. Target for anti-vascular endothelial growth factor (VEGF) receptor therapy. The Oncologist. 2000;5(suppl):32-36.
Madhusudan S, Deplanque G, Braybrooke JP, et al. Antiangiogenic therapy for von Hippel-Lindau disease. JAMA. 2004;291:943-944.
Magee MA, Kroll AJ, Lou PL, Ryan EA. Retinal capillary hemangiomas and von Hippel-Lindau disease. Semin Opthalmol. 2006;21:143-150.
Maher ER, Yates JR, Harries, et al. Clinical features and natural history of von Hippel-Lindau disease. QJM. 1990;77:1151-1163.
Maher ER, Lselius L, Yates JR, Et al. von Hippel-Lindau disease: a genetic study. J Med Genet. 1991;28:443-447.
Shields CL, Shields JA, Barret J, et al. Vasoproliferative tumors of the ocular fundus. Classification and clinical manifestations in 103 patients. Arch Ophthalmol. 1995;113:615-623.
Sigelman J. Retinal diseases. Pathogenesis, laser therapy and surgery. Boston:Little Brown and Company. 1984:316.
Vail D. Angiomatosis retinae, eleven years after diathermy coagulation. Am J Ophthalmol. 1958;46:525-534.
Webster AR, Maher ER, Moore AT. Clinical characteristics of ocular angiomatosis in von Hippel-Lindau disease and correlation with germline mutation. Arch Ophthalmol. 1999;117:371-378.
Wong WT, Chew EY. Ocular von Hippel-Lindau disease: clinical update and emerging treatments. Curr Opin Ophthalmol. 2008;19:213-217.
Wong WT, Liang KJ, Hammel K, Coleman HR, Chew EY. Intravitreal ranibizumab therapy for retinal capillary hemangioblastoma related to von Hippel-Lindau disease. Ophthalmology. 2008;115:1957-1964.
Dr. Finger is a Principal Investigator in the Collaborative Ocular Melanoma Study Group
Collaborative Ocular Melanoma Study Publications: Peer-review papers only.
1. Collaborative Ocular Melanoma Study Group: Accuracy of diagnosis of choroidal melanomas in the Collaborative Ocular Melanoma Study. COMS Report No. 1. Arch Ophthalmol 108:1268-1273, 1990.
2. Collaborative Ocular Melanoma Study Group: Complications of enucleation surgery. COMS Report No. 2. In: Proceedings of the Symposium on Retina and Vitreous (Rudolph M. Franklin, ed.). New Orleans Academy of Ophthalmology. Kugler Publications, New York, 1993; pp. 181-190.
3. Collaborative Ocular Melanoma Study Group: Design and methods of a clinical trial for a rare condition: The Collaborative Ocular Melanoma Study. COMS Report No. 3. Controlled Clin Trials 14:362-391, 1993.
4. Collaborative Ocular Melanoma Study Group: Mortality in patients with small choroidal melanoma. COMS Report No. 4. Arch Ophthalmol 115:886-893, 1997.
5. Collaborative Ocular Melanoma Study Group: Factors predictive of growth and treatment of small choroidal melanoma. COMS Report No. 5. Arch Ophthalmol 115:1537-1544, 1997.
6. Collaborative Ocular Melanoma Study Group: Histopathologic characteristics of uveal melanomas in eyes enucleated from the Collaborative Ocular Melanoma Study. COMS Report No. 6. Am J Ophthalmol 125:745-766, 1998.
7. Collaborative Ocular Melanoma Study Group: Sociodemographic and clinical predictors of participation in two randomized trials: Findings from the Collaborative Ocular Melanoma Study. COMS Report No. 7. Controlled Clin Trials 22:526-537, 2001.
8. Grossniklaus HE, Albert DM, Green WR, Conway BP, Hovland KR for the Collaborative Ocular Melanoma Study Group: Clear cell differentiation in choroidal melanoma. COMS Report No. 8. Arch Ophthalmol 115:894-898, 1997.
9. Collaborative Ocular Melanoma Study Group: The Collaborative Ocular Melanoma Study (COMS) randomized trial of pre-enucleation radiation of large choroidal melanoma. I: Characteristics of patients enrolled and not enrolled. COMS Report No. 9. Am J Ophthalmol 125:767-778,1998.
10. Collaborative Ocular Melanoma Study Group: The Collaborative Ocular Melanoma Study (COMS) randomized trial of pre-enucleation radiation of large choroidal melanoma. II. Initial mortality findings. COMS Report No. 10. Am J Ophthalmol 125:779-796,1998.
11. Collaborative Ocular Melanoma Study Group: The Collaborative Ocular Melanoma Study (COMS) randomized trial of pre-enucleation radiation of large choroidal melanoma. III. Local complications and observations following enucleation. COMS Report No. 11. Am J Ophthalmol 126:362-372, 1998.
12. Collaborative Ocular Melanoma Study Group: Echography (ultrasound) procedures for the Collaborative Ocular Melanoma Study. COMS Report No. 12. J Ophth Nurs Technol Part I, 18(4):143-149, Part II, 18(5):219-232, 1999.
13. Collaborative Ocular Melanoma Study Group: Consistency of observations from echograms made centrally in the Collaborative Ocular Melanoma Study. COMS Report No. 13. Ophthalmic Epidemiol 9:11-27, 2002.
14. Collaborative Ocular Melanoma Study Group: Cause-specific mortality coding: Methods in the Collaborative Ocular Melanoma Study. COMS Report No. 14. Control Clin Trials 22: 248-262, 2001.
15. Collaborative Ocular Melanoma Study Group: Assessment of metastatic disease status at death in 435 patients with large choroidal melanoma in the Collaborative Ocular Melanoma Study. COMS Report No. 15. Arch Ophthalmol 119:670-676, 2001.
16. Collaborative Ocular Melanoma Study Group: Collaborative Ocular Melanoma Study (COMS) randomized trial of I-125 brachytherapy for medium choroidal melanoma. I. Visual acuity after 3 years. COMS Report No. 16. Ophthalmology 108(2):348-366, 2001.
17. Collaborative Ocular Melanoma Study Group: The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma. II. Characteristics of patients enrolled and not enrolled. COMS Report No. 17. Arch Ophthalmol 119: 951-965, 2001.
18. Collaborative Ocular Melanoma Study Group: The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma. III. Initial mortality findings. COMS Report No. 18. Arch Ophthalmol 119: 969-982, 2001.
19. Collaborative Ocular Melanoma Study Group: The COMS randomized trial of iodine 125 brachytherapy for choroidal melanoma. Local treatment failure and enucleation in the first 5 years after brachytherapy. COMS Report No. 19. Ophthalmology 198:2197-2206, 2002.
20. Collaborative Ocular Melanoma Study Group: Trends in size and treatment of recently diagnosed choroidal melanoma, 1987-1997. Findings from patients evaluated at Collaborative Ocular Melanoma Study centers. COMS Report No. 20. Arch Ophthalmol 121:1156-1162, 2003.
21. Collaborative Ocular Melanoma Study Group: Comparison of clinical, echographic, and histologic measurements from eyes with medium-sized choroidal melanoma in the Collaborative Ocular Melanoma Study. COMS Report No. 21. Arch Opthalmol 121:1163-1171, 2003.
22. Collaborative Ocular Melanoma Study Group: Ten-year follow-up of fellow eyes of patients enrolled in Collaborative Ocular Melanoma Study (COMS) randomized trials. COMS Report No. 22. Ophthalmology 111:996-976, 2004.
23. Diener-West M, Reynolds SM, Agugliaro DJ, Caldwell R, Cumming K, Earle JD, Green DL, Hawkins BS, Hayman I, Jaiyesimi I, Kirkwood JM, Koh W-J, Robertson DM, Shaw JM, Thoma J. Screening for metastasis from choroidal melanoma: Experience of the Collaborative Ocular Melanoma Study. Collaborative Ocular Melanoma Study Report No. 23. Am J Clin Oncol 22:2438-2444, 2004.
24. Collaborative Ocular Melanoma Study Group. The Collaborative Ocular Melanoma Study (COMS) randomized trial of pre-enucleation radiation of large choroidal melanoma. IV. Ten-year mortality findings and prognostic factors. COMS Report No. 24. Am J Ophthalmol 138:936-951, 2004.
25. Melia BM, Moy CS, McCaffrey L: Quality of life in patients with choroidal melanoma: A pilot study. Ophthalmic Epidemiol 6:19-28, 1999.
26. COMS Quality of Life Study Group: Quality of life assessment in the Collaborative Ocular Melanoma Study: Design and methods. COMS-QOLS Report No. 1. Ophthalmic Epidemiol 6:5-17, 1999.
27. COMS Quality of Life Study Group: Development and validation of disease-specific measures for choroidal melanoma. COMS-QOLS Report No. 2. Arch Ophthalmol 121:1010-1020, 2003.
28. Collaborative Ocular Melanoma Study Quality of Life Study Group. Quality of life after iodine 125 brachytherapy versus enucleation for choroidal melanoma: 5-year results from the Collaborative Ocular Melanoma Study prospective study. COMS-QOLS Report No. 3. Arch Ophthalmol (under revision for resubmission, July 2004).
29. Collaborative Ocular Melanoma Study Group: The Collaborative Ocular Melanoma Study (COMS) randomized trial of pre-enucleation radiation of large choroidal melanoma. IV. Ten-year Mortality findings and prognostic factors. COMS Report No. 24. Am J Ophthalmol 138:936-951, 2004.
30. Collaborative Ocular Melanoma Study Group: Second Primary Cancers after Enrollment in the COMS Trials for Treatment of Choroidal Melanoma. COMS Report No. 25. Archives of Ophthalmology 2005:123:601-4.
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.