About Choroidal Melanoma
About Enucleation Surgery
Frequently Asked Questions after Enucleation Surgery
How do I choose an eye cancer specialist?
Enucleation: About Ocular Prosthesis Care
Ophthalmic Radiation Therapy
Should I get a second opinion?
What about Retinoblastoma?
About Choroidal Melanoma
Q: Can the laser be used to treat an eye melanoma?
A: Most studies have shown that the laser treatment just burns the surface of the melanoma. This can leave live cancer cells under the tumor’s laser scarred surface and in the wall of the eye. It may be just a matter of time before the cancer will grow again. If the cancer is not killed or removed, there is a chance that it might spread to the rest of your body.
Due to the high incidence of failure using Transpupillary Thermotherapy (TTT) laser alone, it is rarely used without additional plaque radiation for choroidal melanoma. However, intraocular hemorrhages are common, and in rare cases the wall of eye (sclera) can be weakened allowing tumor growth into the tissues behind the eye.
In contrast, TTT laser is commonly successful in treatment of small retinoblastomas.
Related Links
Q: Can you surgically remove the tumor and leave my eye?
A: During this type of surgery the eye must be opened. Though not a proven risk for metastasis, eye wall resection allows tumor cells to float out of the eye and into the orbit (spaces around the eye).
With lamellar (split thickness) eye wall resection, the wall of the eye (sclera) is sewn back in place. The COMS study showed that up to 50% of choroidal melanomas had invaded the wall of the eye. Therefore, with lamellar eye wall resection, the entire tumor is not always removed or treated. In order to prevent recurrence, eye cancer specialists are currently adding plaque therapy to treat the eye wall. Lastly, depending on the skill of the operating surgeon, many eyes do not tolerate eye wall resection. These eyes suffer sight limiting retinal detachment, cataract, and intraocular hemorrhage.
Q: How long will I have to be a patient?
A: For the rest of your life. You must be followed by an eye-care specialist and may need a medical oncologist. You may want to consider this when choosing your doctors and their location.
Patients who receive plaque radiotherapy are typically seen by their eye care specialist every 3 to 4 months. Patients may undergo twice-yearly blood tests, radiographic imaging studies and physical examinations. Patients being treated for radiation retinopathy and/or optic neuropathy may have to be seen every 4-6 weeks.
Copies of your laboratory evaluations should be forwarded to your eye cancer specialist’s office, so they can be double-checked for metastatic disease. In the United States, the law requires that you must request this in writing from your family doctor, internist, or oncologist.
Q: How will having a choroidal melanoma affect my life?
A: Almost all patients who have been determined to have an ocular tumor (e.g. choroidal melanoma) are treated and then return to their normal activities.
The time between the diagnosis and the completion of treatment can be very stressful. Rely on your doctors and family for help. After you are treated they should encourage you to get back to your normal activities. Just remember to be periodically monitored by your eye care specialists and general medical doctors.
Q: What are the standard treatment options?
A: Standard treatments for choroidal melanoma are enucleation and radiation.
Enucleation means removal of the eye. In most cases, it is the only form of treatment that allows your doctor to completely remove the tumor from your body. Unfortunately, patients also lose their vision and the cosmetic use of the eye. With time, almost all patients are able to do all the things they used to before losing their eye. Since the COMS study found no difference in survival between enucleation and plaque radiation therapy (for medium-sized melanomas), few doctors will recommend enucleation if “eye-sparing” radiation therapy is possible.
The most common alternative to removal of the eye is radiation therapy, and the most commonly used radiation technique for intraocular melanoma is eye-plaque radiation therapy.
Plaque technique involves placing a dish-shaped plaque-device (about 1 to 2 centimeters in diameter) on the outer surface of the eye, under the tumor. The plaque is implanted behind the eye, left in place for up to 5-7 days, and then removed. During treatment patients are likely to notice no more than occasional discomfort.
The effects of radiation on the tumor are typically measured 3 to 4 months after treatment. Eventually, eye melanomas shrink to about 40% of their pretreatment size. Though they rarely disappear, these tumors are considered to be dead. In most studies, irradiated tumors will regrow (within the eye) in less than 8% of cases. Local control means the tumor was killed. Ask your doctor about their rates of local control after treatment and for how long those patients were followed (typically reported at 5 and 10 years after treatment). You can see The New York Eye Cancer Center’s local control rates on our outcomes page.
Note about radiation: More than 95% of patients have no problems associated with plaque surgery. As with any ocular surgery, there can be secondary retinal detachments, hemorrhages, or infections. There are also the regular risks related to hemorrhage, infection or reaction to anesthesia. Most plaque patients do not develop these problems.
Q: What research is being done for ocular melanoma?
A: Around the world, researchers are working on new methods of diagnosis and treatment for choroidal melanoma, retinoblastoma, and other ocular tumors. One only has to do a PubMed search to find thousands of published articles.
It is important to point out two major research initiatives:
The first multi-center, multinational prospective randomized clinical study carried out for an eye cancer was called The Collaborative Ocular Melanoma Study (COMS). These types of studies offer the best evidence-based statistically significant information currently available. The National Eye Institute (NEI) and the National Institute of Health (NIH) supported the COMS.
The COMS had three studies:
- The Small Choroidal Melanoma Study confirmed that orange pigmentation, leakage of fluid, and thickness are all correlated to tumor growth and metastatic potential. This study also found that there exists a risk of metastatic melanoma from small choroidal melanomas.
- The Medium-Sized Choroidal Melanoma Study determined that plaque radiation was equal to removal of the eye for the prevention of metastatic choroidal melanoma.
- The Large-Sized Choroidal Melanoma Study determined that 2000 cGy of external radiation prior to enucleation does not prevent the spread of choroidal melanoma.
The second major collaborative step forward was when The American Joint Committee on Cancer joined with the International Union Against Cancer to develop a Tumor-Node-Metastasis (TNM) grading system for most eye cancers. It is our hope that this common language will enable centers (around the world) to compare their results.
Read more about the COMS here.
Q: What usually happens to a patient’s vision after treatment?
A: Enucleation
After enucleation (removal of the eye) there is no vision from that eye. The patient is considered monocular and sees from the remaining eye. Most patients see well from their remaining eye and live normal lives. Loss of one eye does affect depth perception, but with time, most patients are able to adjust. Consider that part of depth perception comes from the relative size of objects (distant objects appear smaller).
A: Plaque Radiation Therapy
Prior to treatment for radiation-related damage to the retina and optic nerve, post-plaque radiation therapy for choroidal melanoma caused vision loss in half of patients within 5 years. However, with the use of laser treatment and/or intraocular anti-VEGF drug therapy, the vision destroying radiation retinopathy can be suppressed. Anti-VEGF suppression of radiation retinopathy and optic neuropathy has preserved patient vision for years. Further, the natural eye looks and moves better than an ocular prosthesis.
Disadvantages of plaque versus enucleation include that you must see an ophthalmologist every 3 to 4 months after treatment for dilated ophthalmoscopy and ultrasound measurements of your tumor. This is because patients who have their eye irradiated (plaque or proton) develop radiation complications within the eye, and there is a small chance that the tumor might regrow.
The patient’s chance for functional vision after radiation is related to how close the tumor is to the functional center of the retina (macula), the type of radiation, and the dose delivered to normal ocular structures. The American Brachytherapy Society Consensus Guidelines suggest that all centers perform pre-operative comparisons of plaque types for dose to normal eye structures.
To learn more about radiation treatments, read the radiation therapy section of this web site.
Q: Will the tumor spread to other parts of my body?
A: Less than 4% of patients are found to have metastatic melanoma at the time of diagnosis. But with time after treatment, a much larger percentage are found to develop metastasis. This difference is thought to be due to undetectable microscopic melanoma cells present at the time of treatment. It is not helpful to dwell on percentages, but your doctor should be able to give your approximate chance of developing metastasis based on your tumor’s size and location.
About Enucleation Surgery
Q: If I must lose my eye, will it hurt?
A: The eye is surrounded by bones; therefore, it is much easier to tolerate removal of an eye as compared to loss of a lung or kidney.
Almost all enucleation surgery can be performed as an outpatient. Older patients and those with significant systemic medical problems may have to stay in the hospital after surgery.
Since this surgery is usually performed under general anesthesia, the patient does not feel or see anything during surgery. Long-acting local anesthesia (6 hours) can be given during surgery, allowing for the least amount of pain possible (when you wake up in the recovery room). Most patients who have their eye removed have a mild headache for 24-36 hours after surgery.
Q: What is enucleation?
A: Enucleation is removal of the eye. It is the form of treatment that allows your eye cancer specialist to remove the tumor from your body. Unfortunately, patients also lose all the vision and the cosmetic use of the eye. With time, almost all patients are able to do most all the things they used to do before their eye was removed.
Q: What might I look like after enucleation?
A: This is a patient who has completed cosmetic rehabilitation after enucleation surgery. Notice that he looks normal, but the prosthetic eye does not move as well as a normal eye.

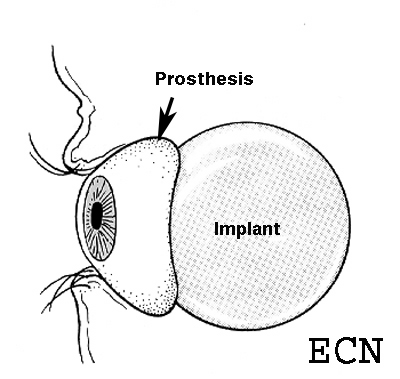
Q: When will I get a prosthetic eye?
A: Patients can usually have a temporary prosthesis (that looks like an eye) within 10 days of enucleation surgery. Besides the swelling and the “black-eye,” you will look fairly normal. After a final prosthetic fitting, 90% of patients are happy with the way they look, and 80% say others can’t even tell they are monocular.
Read the book A Singular View, by Frank Brady. It will help in your transition. This book was written by an airplane pilot who lost one eye. We suggest that you wear unbreakable polycarbonate glasses to protect your good eye.
Q: Why are very large-sized tumors treated by removal of the eye?
A: This is because the amount of radiation required to kill a large tumor that fills most of the eye is just too much for the eye to stand. Within months to years, many patients who are treated with radiation for very large ocular melanomas lose vision, develop glaucoma, or have their eye removed anyway. It is important that the eye cancer specialist inform each patient regarding their approximate chance of developing radiation associated complications. Despite these risks, more and more patients with large intraocular tumors are treated with eye and vision-sparing radiation therapy.
Frequently Asked Questions After Enucleation Surgery
Q: How long will I have to be a patient?
A: For the rest of your life. You must be followed by an eye-care specialist and may need a medical oncologist. You may want to take this into account in choosing your doctors and their location.
An eye care specialist examines patients who are enucleated twice a year. In addition, patients should have blood tests, radiographic imaging studies, and physical examinations. Copies of your laboratory evaluations should be forwarded to your eye-cancer specialist’s office so they can be double-checked for metastatic disease. The law requires that you must request this in writing from your family doctor, internist, or oncologist.
Q: How often will I need to be checked after enucleation?
A: Dr. Finger recommends that you have an eye examination within 1 week, 1 month, and at least every 6 months after surgery. This is to monitor for inflammation or infection, and because there is an extremely small chance the tumor will regrow behind your prosthesis.
Dr. Finger recommends that you return for a complete ophthalmic oncology examination at least on a yearly basis. You should also have twice-yearly medical check-ups by your family doctor, internist, or medical oncologist.
Q: What sort of care will my eye need after I go home?
A: You will be advised to take topical antibiotic and steroid medications for one month. These medicines will help you heal more safely and quickly.
For the first week after surgery, you will tear a lot. These tears may contain a little blood. This is normal. Once a day, you should gently wash the outside of your eyelid with a warm, clean, soapy washcloth. Don’t let matter accumulate to form a crust on your eyelids.
Q: What will happen to my vision?
A: Enucleation means removal of the eye. It is a form of treatment that completely removes the primary tumor from the body, but the patient loses all vision and the cosmetic use of the eye. It takes some time to adjust to using one eye, but almost all patients learn to compensate within the first year after surgery.
Q: When can I get a prosthesis?
A: Dr. Finger can usually place a temporary prosthesis (that looks like an eye) within 10 days of enucleation surgery. Most patients are fitted with a permanent prosthesis 4 to 6 weeks later.
Q: When can I go back to normal activity?
A: Do not lift, strain, or rub your eye for at least 14 days after surgery.
Do not take aspirin or other blood thinners unless your internist says it is required. The orbit should heal quickly, and you should be able to return to school or work within 2 to 6 weeks after surgery.
Q: When can I wash my hair and face?
A: You should gently clean your lids each day. You may use a clean wash cloth and baby shampoo. You should not rub your eyelids or run the shower at your operated eye for at least 10 days after surgery.
How do I choose an Eye Cancer Specialist?
Q: How do I pick a doctor?
A: You should pick a doctor who has experience caring for eye cancer patients and with whom you are comfortable. You should be able to ask questions about your case and feel comfortable that your treatment decisions are not only based on available science, but also take into account your personal situation and medical problems. Since you may need to see your doctors for many years, consider that it is easier to be treated and followed with a doctor in your area.
Consider the following:
- You should be guaranteed to see the doctor with whom you are making the appointment (not a substitute doctor). Ask when making your appointment.
- Make sure that your surgeries will be performed by the doctor you want. Ask the doctor who will be performing your surgery when signing your consent form.
- You should be able to ask questions about your case and treatment decisions.
- Ask how easy it is to speak with your doctor before and after surgery.
- Ask what happens when there is an emergency during nights and weekends.
- Make sure your doctor has the expertise to manage any eye and/or systemic problems you may have in the future.
Q: How long will I have to be a patient?
A: For the rest of your life. You must be followed by an eye cancer specialist and may need a medical oncologist. You may want to take this into account when choosing your doctors and their location. Patients who receive plaque radiotherapy are typically seen every 3-4 months. Patients who are enucleated are usually seen twice a year. Many eyelid and orbital tumor patients are advised to follow up with their eye cancer specialist, at least, on a yearly basis.
In any case, your eye care specialist should check to make sure that you have regularly scheduled medical workups, including an evaluation for metastatic disease (as necessary). Copies of your laboratory evaluations should be forwarded to your eye-cancer specialist’s office so that they can be double-checked. The law requires that you must request this in writing from your family doctor, internist, or oncologist.
Enucleation: About Ocular Prosthesis Care
Q: How do I remove my prosthesis?
1) First, wash your hands.
2) Then you should place a towel over your lap or sink to act as a net for the prosthesis if it slips out of your hand. Should it fall it could scratch, break, or get lost.
Manual Technique
3) Place one finger on the temporal (towards the ear) aspect of the lower lid on top of the cheek bone.
4) Look up.
5) Cup your other hand under your eye (to catch the prosthesis).
6) Gently press your finger in and pull the eyelid skin towards your ear (on that side).
7) The edge of your prosthesis will likely be emerging at the edge of the lower eyelid, or (less likely) it has fallen into your cupped hand.
8) If the prosthesis is just barely out, you can use a finger on your other hand to rotate it out of the socket.
9) Don’t be surprised if some discharge comes along with the prosthesis.
Suction Technique
1) Hard contact lens suction devices are commercially available in drug stores and vision centers.
2) These devices can be squeezed to create a vacuum that attaches the device to the front of the prosthesis.
3) Once attached, the patient can lift the bottom portion of the prosthesis out from beneath the lower lid, then slide the superior portion down towards the cheek.
Once the Prosthesis Is Out
1) Commercially available sterile saline solution should be used to clean your eye socket.
2) Now you can consider cleaning the prosthesis.
Q: How do I clean my prosthesis?
1) Place the prosthetic eye into a container that can be filled with liquid as to cover the prosthesis.
2) Full or half strength hydrogen peroxide solution can be used to soak the prosthesis for 10 to 15 minutes. After soaking, remove the prosthesis from the container and rinse it with sterile saline solution.
3) Prosthesis cleaning is typically performed once or twice a week (as instructed by your eye care professionals).
4) Continuous and consistent periodic cleaning of the prosthesis will increase your comfort, decrease secretions, prevent secondary conjunctivitis and extend the life of your ocular prosthesis.
Q: How often do I need to have my prosthesis professionally cleaned or replaced?
1) You should return to your ocularist for professional cleaning and polishing 2 times each year.
2) Most patients get a new prosthesis every 3 to 5 years because even with excellent maintenance, the tissues around the prosthesis can change and the artificial eye can become scratched.
Warning!!!
If you notice excessive discharge, swelling or irritation, you should call your eye care professional immediately.
Related Links
For the more medically minded, you can go to a medical library, or click and order a copy of our comprehensive review of:
Ophthalmic Radiation Therapy
Q: Am I radioactive after the plaque is removed?
A: No! Once the radiation plaque is removed, all the radioactivity is gone. There will be no radiation left in your body, your clothing, your glasses, or any of your personal belongings. However, the effects of the radiation delivered to your tumor and eye will continue to be observed for months and years after treatment.
Q: How often will I need to be checked after plaque treatment?
A: We recommend that you be examined every 3-4 months after plaque radiation. This is because there is a small chance the tumor will regrow or that your eye may develop radiation-related problems (that may require treatment).
In addition to seeing your local eye care specialist, we recommend that you return for a complete ophthalmic oncology examination (at least) on a yearly basis.
You should also have twice-yearly medical check-ups by your family doctor, internist, or medical oncologist. Dr. Finger recommends that you have a medical checkup at least two times a year. This should include a physical examination and radiographic imaging of the abdomen.
Q: How quickly will my tumor go away after plaque radiation?
A: Tumors are usually measured to shrink after 3 months. We don’t measure a tumor before three months, because they can swell and become temporarily larger after radiation, unnecessarily frightening patients. Since the goal of radiation therapy is to prevent the tumor from growing, don’t be concerned if your tumor shrinks slowly. Most tumors eventually shrink to about 40% of their original size and rarely disappear. A residual lump of dark, shrunken tumor typically persists for years after treatment.
Q: How soon can I return to normal activities?
A: The eye should heal quickly. You should not lift any objects greater than 10 pounds or rub your eye for at least two weeks after surgery. Then you can return to normal activity. Patients usually return to school or work within 2-4 weeks after completion of treatment. If the tumor has caused a retinal detachment, it may take longer for you to return to normal activities.
Q: What after-care will my eye need after I go home?
A: After ophthalmic plaque radiation therapy, the patient is usually requested to take eye-drops daily for about a month. These drops contain antibiotics, steroids, and medicines to relax your eye. These drops help your eye heal more safely and quickly. For the first week after surgery, you will tear and the tears may contain a little blood. This is normal. You should gently wash the outside of your eyelid with a warm, clean, soapy wash cloth. Don’t let matter accumulate to form crust on your eyelids.
Q: What are the differences between Protons versus Plaques?
A: Proton Beam Radiotherapy is a form of external beam irradiation. It involves directing radiation through the front of the eye, lids, and orbit in order to reach the intraocular tumor. Eyelash loss, eyelid excoriation, corneal neovascularization and ulceration, dry eye, neovascular glaucoma, and cataract have been reported to be more common after proton beam radiation therapy.
Proton beam radiation therapy typically requires surgical clips to be sewn onto the eye (around the tumor) this helps the radiation therapist to direct the beam into the eye. Eye movements are monitored on a video screen because if the eye moves, the beam moves away from the tumor. If the eye is detected to move, the radiation technologist will temporarily turn off the beam until the eye is repositioned. In contrast, radiation eye plaques are sewn onto the eye as to cover the base of the intraocular tumor. So when the eye moves, so does the plaque. With eye plaque, eye movement is not thought to appreciably affect the distribution of radiation within the eye.
Both proton beam and Fingers’ slotted plaques can be used to treat certain tumors that are near, touch or even surround the optic nerve.
Eye-Plaque Radiotherapy typically involves attaching a dish-shaped radiation source beneath the tumor and leaving it there for 5-7 days. With proton beam, once the marking clips are surgically placed, the patient visits the radiation center for 3-5 treatments. The marker-clips are not typically removed.
Compared with Proton-Beam, the front of the eye usually receives much less radiation with plaque radiation therapy, but parts of the retina may receive more. This is why anterior “front of the eye” complications are much less commonly reported after low-energy ophthalmic plaque radiation therapy.
Q: What is a radioactive eye-plaque?
A: A radioactive eye-plaque is a device that can be used to deliver a high-dose of radiation to an intraocular tumor.
This is because when an eye-plaque contains radioactive iodine-125 or palladium-103 seeds, the gold of the plaque blocks more than 99% of radiation. Therefore, when the plaque is sewn to the outside of your eye (underneath the tumor), the radiation is directed into the eye. For an average-sized tumor, less than 10% of the radiation makes it out of the other side of the eye.
Plaques come in various sizes (diameters between 10 to 22 mm). A plaque will be chosen to cover your entire tumor plus at least a 2-millimeter “safety margin”. The extra area is included to make sure the entire tumor is within the targeted area. The plaque is implanted utilizing several standard techniques (transillumination, ophthalmoscopy and ultrasound). Intraoperative ultrasound imaging and light-assisted plaque localization are techniques developed to make plaque-placement more accurate (see innovations).
Radiation treatment is continuous and will typically take up to 7 days. At the end of treatment, your tumor will have been given all the necessary radiation. Once your plaque is removed, there will be no radioactivity left in your body.
Radioactive plaques come in various sizes with suture eyelets so that it can be temporarily attached to the wall of the eye for treatment.
Q: What is plaque radiation therapy?
A: Radioactive plaque therapy is a form of treatment, which allows the eye-cancer specialist to destroy your tumor without removing the eye. Unfortunately, the radiation can also affect the normal parts of your eye and harm your vision. Your ophthalmic and radiation oncologists will work together to try to increase the effectiveness of radiation (to kill your cancer), while decreasing the chance that radiation will harm the normal parts of your eye.
Q: What is proton beam radiation therapy?
A: Protons are charged nuclear particles that can be sent into the eye. These particles travel through and are somewhat absorbed by tissues on the way to your intraocular tumor. The targeted zone (the tumor and surrounding 2-3 mm) gets most of the radiation. The proton radiation field is in the shape of a tube, with little side-scatter or dose posterior to the eye. Like plaque radiotherapy, the amount of radiation to the normal parts of the eye depends of the size and location of the tumor.
Q: What radiation precautions must be taken?
A: While the radiation-plaque is sewn onto your eye, certain precautions must be observed. These rules will ensure that visitors and patients in surrounding areas do not receive radiation exposure in excess of the Nuclear Regulatory Commission (NRC) regulations. A list of rules are given to you before you go home with the plaque in place and can be disregarded after you have the radiation-plaque removed.
Q: What will happen to my vision?
A: Radiation may cause eventual blurring, dimming, or rarely a total loss of vision (in the eye with the tumor). The amount of vision loss depends on what your vision was before treatment, how close the tumor is to the center of your retina (the fovea), and how sensitive your tissues are to radiation. Most plaque-irradiated eyes maintain some central vision, and almost all retain peripheral vision. Plaque radiation should not affect the vision in the other eye.
Q: Why does the plaque stay in place for up to 7 days?
A: Plaque radiation therapy is delivered over to a dose known to destroy the cancer, and at a dose rate that will be tolerated by the eye. The rate at which the radiation is delivered is affected by both the radiation source and the size of the tumor.
In consultation with the radiation oncologists, eye plaques are individually designed and constructed for each patient. Specialized computer programs are used to calculate the total dosage and speed of radiation. The precise distribution of radiation throughout the eye is calculated and used to determine the risks of secondary radiation complications.
Q: Will my hair fall out from radiation?
A: It is normal for patients to have fears about radiation.
The type of radiation used in most eye plaque therapy should not cause hair loss, nausea, brain damage, or affect your other eye.
Other forms of radiation therapy can cause hair loss within the field of irradiation. For example, proton beam radiation therapy is associated with eyelash loss. External beam therapy can also cause hair loss where it enters and exits the head.
Q: Should I Get a Second Opinion?
A: Second opinions are great when all your doctors say the same thing. Unfortunately, differing opinions can make things even more confusing. Remember to ask the doctor:
- What are the standard treatment options for my tumor?
- If the proposed treatment is “new” or investigational? If so, how many patients have been treated? How long have they been followed for recurrent disease?
- What have your doctor’s results been for tumor control and vision retention?
- Is the proposed treatment FDA or CE approved?
- Who will be the operating surgeon? In the case of plaque therapy; who will put it in and who will take it out?
- Does your center compare radiation plaque types (before surgery) to determine which one would be best for my tumor?
- Does your center keep plaque patients in the hospital or send them home during treatment and why?
- Does your eye cancer specialist and center personally follow treated patients for recurrence and metastatic disease?
- How soon will you ask me to return after surgery?
- What tests do you perform (over time) to monitor my body for metastatic disease?
- What does your eye cancer specialist do if I am found to have metastatic disease?
What About Retinoblastoma?
Q: Until what age can a child develop another retinoblastoma?
A: Most retinoblastomas are diagnosed before the age of 3. Most eye cancer specialists agree that a child with retinoblastoma is not likely to develop a new tumor after 7 years of age.
Q: What are the most common symptoms of retinoblastoma?
A: Most children are found to have a white pupil “leukocoria,” or a deviated eye “strabismus,” or secondary painful glaucoma. In less developed countries patient more commonly present with orbital or optic nerve extension or metastasis.
Q: What other eye diseases can cause leukocoria “white pupil?”
A: Other than retinoblastoma, cataract, Coat’s disease, persistent hyperplastic primary vitreous, and retinopathy of prematurity can cause the appearance of a white pupil.
Q: Who gets retinoblastoma?
A: There are typically 325 of new cases of retinoblastoma diagnosed each year in North America. Ten thousand cases are estimated to occur throughout the world. Retinoblastoma occurs equally in boys and girls, different ethnic groups, and in either eye.
Retinoblastoma is a genetic cancer. Therefore, 10% of patients will have a family history of retinoblastoma, and 25% will affect both eyes. Forty percent of patients have the retinoblastoma gene throughout their body. The abnormal gene is 13q14.2, that is chromosome 13, long arm (q), band 14.2. Though it is the most common primary intraocular cancer in children, intraocular leukemia is more common.








