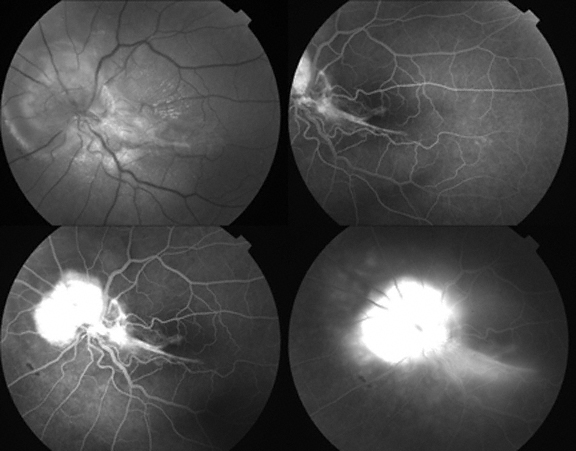
Color Photographs: Juxtapapillary Capillary Hemangioma
Dr. Soarnil would appreciate suggestions as to treatment options to optimize visual outcome without risk to this 42 year old woman with a juxtapapillary hemangioma.
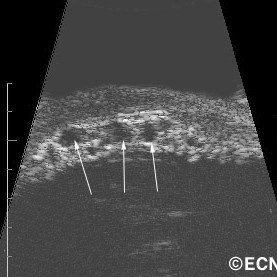
“This is a case of juxtapapillary capillary hemangioma in a patient with V-H-L Disease, a woman 42 yo. She came to my clinic in February 2007, presenting a VA 20/20 in both eyes, no capillary hemangiomas in the RE and a juxtapapillary hemangioma in the left eye, asymptomatic. After 6 months, she started having visual symptoms and exudates (Top) and we performed TTT treatment. Exudates decreased, but an epiretinal membrane appeared. Hemangioma activity persisted, and a second TTT was performed December 2007, and ERM symptoms worsened and the hemangioma persisted.
View the fluorescein angiogram taken after TTT – treatment
Flourescein Angiography of the juxtapapillary hemangioma
What do you think is the next step? Intravitreal injection of anti- VEGF? Vitreoretinal surgery with endophotocoagulation ? Brachytherapy? Any combination? I will appreciate very much your suggestions.
This patient was also noted to have a pigmented iris tumor in his right eye.
Impression
Posterior Iris Pigment Epithelial Cyst
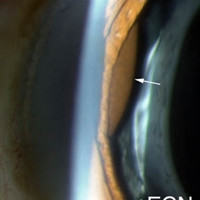
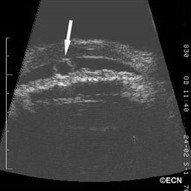
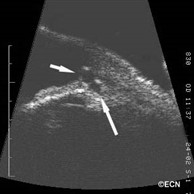
Iris pigment epithelial cysts are typically located behind the iris stroma. As they expand, the cyst wall comes in contact with the natural lens (or IOL) posteriorly and push the iris stroma anteriorly. Gonioscopy and high-frequency ultrasound examination usually reveals focal angle closure. Since most of the trabecular meshwork remains open, most patients do not develop narrow angle glaucoma.
Giant iris pigment epithelial cysts can cause total angle closure warranting intervention. These patients have been treated with Yag-laser iridotomies or surgical iridectomy.
Almost all iris pigment epithelial cysts can be monitored with periodic observation for evidence of secondary glaucoma. Slit-lamp photography, gonioscopy and high-frequency ultrasonography are particularly helpful in evaluating for progressive enlargement. The natural history of iris pigment epithelial cysts is poorly understood.
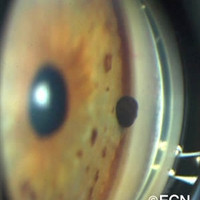
This digital image shows a rounded pigmented tumor extending from the anterior chamber angle.
This patient was noted to have a pigmented tumor on his right iris.
The digital images below will show a rounded pigmented tumor extending from the anterior chamber angle. Gonioscopy revealed no evidence of pigment dusting around the tumor or tumor in the adjacent ciliary body. It was also significant that there was no evidence of distortion of the iris stroma, ectropion uveae, sector cataract or abnormal vascularity (as might be seen with iris melanoma).
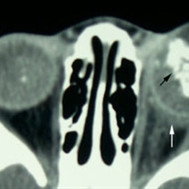
A 63 year old male was referred to The New York Eye Cancer Center with a 6 month history of progressive painless proptosis of the right eye.
These magnetic resonance imaging (MRI) studies demonstrate displacement of the optic nerve, a bright T1 tumor image, and a variably bright T2 tumor image. The tumor is noted to involve the orbit, the ethmoid and frontal sinuses.
Despite this large orbital tumor with optic nerve displacement, the patient was 20/20 OU, he had no visual field defect, and no signs of optic neuropathy. A complete medical survey was initiated and the patient was cleared for surgery. A combination of anterior orbitotomy and transnasal ethmoidectomy were performed to evacuate the mucus and allow for future drainage.
Though recurrence is possible, this surgery is typically curative. We recommend sending the mucoid contents for culture and sensitivity and cytopathology.
A 67 year old male was referred to The New York Eye Cancer Center with a 18 x 18 mm base, and 9.3 mm high dome-shaped tumor in his left eye.
A dynamic 10 MHz ultrasound reveals the “twinkling” of blood as it flows within a choroidal melanoma.
Note
This is a large file which may take up to 5 minutes to download (at 56K). If you are using dial-up Internet access, you will see a static image for 5 minutes.
Note the “twinkling” within the tumor.
This is caused by blood circulating within the melanoma. You can use this observation to differentiate between benign and malignant tumors. In general, malignant tumors have an active circulation as compared to “pseudo-melanomas” like a choroidal hemorrhage. The “twinkling” represents intrinsic vascularity or blood flow. Blood flow and vascularity will be found to diminish after radiation therapy.
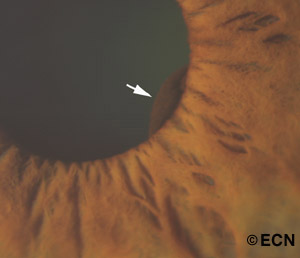
Note the pigmented tumor presenting at the pupillary margin (arrow).
A 64-year-old female was referred to The New York Eye Cancer Center with a small iris tumor visible at the pupillary margin
Impression
Iris Pigment Epithelial Cyst
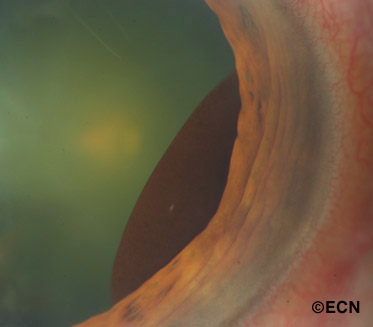
Iris pigment epithelial cysts are commonly located at the iridociliary junction and are round or oval. When observed by slit-lamp examination, they have a smooth brown surface. Visualization of the tumor can be improved by dilation of the pupil.
The iris pigment epithelial cyst seen after dilation of the pupil.
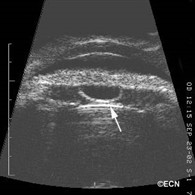
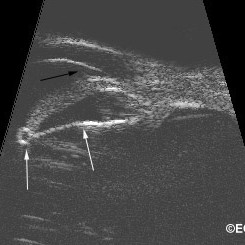
Iris pigment epithelial cysts have thin walls and sonolucent contents (as imaged by UBM). It is generally accepted that the high reflectivity of the cyst wall is caused by its epithelial cell lining and that its sonolucent core is consistent with a liquid content.
Iridociliary cysts typically displace the iris root anteriorly. This can induce a focal plateau-iris configuration with or without angle-closure. Though single cysts are more common, multiple cysts are found in at least one third of cases. When multiple cysts involve more than 180 degrees of the iris, as it does in 10% of patients, angle-closure glaucoma may develop.
The natural history of iris pigment epithelial cysts is poorly understood. Therefore serial observation is warranted.
Recommendation:
Observation
Laser cystotomy for progressive angle closure, threatening acute glaucoma
References
Differential Diagnosis of Anterior Segment Cysts by Ultrasound Biomicroscopy. Authors: Marigo FA, Esaki K, Finger PT, Greenfield DS, Liebmann JM, Ritch R. Ophthalmology 1999;106:2131-35
Anterior Segment Tumors: Current Concepts and Innovations. Marigo FA, Finger PT. Survey of Ophthalmology 2003;48:569-593.
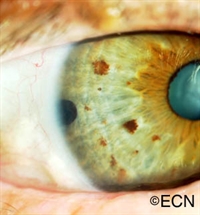
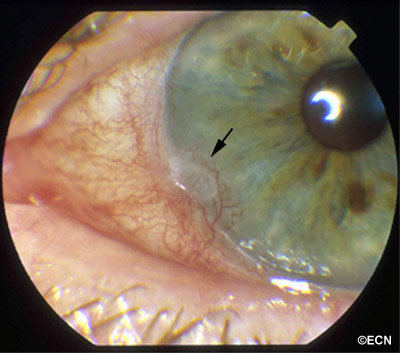
There was keratinization of the overlying corneal epithelium, corneal neovascularization, and punctate keratopathy (arrow).
A 71-year-old white female presented with a growth which appeared on her left eye 3 months prior to examination. Slit lamp examination revealed a gray, gelatinous, slightly elevated neovascular mass measuring 2.4 x 3.6 mm at the limbus centered in the 8 o’clock meridian.
An exfoliative biopsy was performed and a plug was placed in the lower punctum. Histopathology confirmed the diagnosis of CIN (corneal and conjunctival intraepithelial neoplasia).
The known risks and potential benefits of topical Interferon Alfa-2b (IFNa2b) and traditional forms of treatment (including but not limited to surgical excision and cryotherapy) were extensively discussed. After informed consent was obtained, treatment was given with topical IFNa2b (Schering Plough, Kenilworth, NJ).
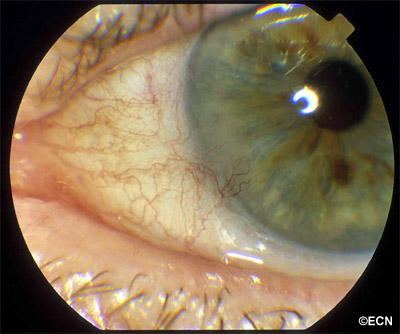
Three Month Follow-up Photograph – Dose Given = 1 million units/cc, 1 drop, four times daily. She was followed biweekly and by the 3-month follow-up, the lesion had completely resolved. At 15 months of follow-up, there has been no recurrence.
Treatment of CIN has traditionally involved wide excision of the tumor with application of cryotherapy, topical Mitomycin-C, or radiation.
At The New York Eye Cancer Center, currently almost all patients with squamous conjunctival neoplasia can be treated without surgery, using topical chemotherapy eye drops. Depending on the type of chemotherapy eye drops, there may be local side effects (conjunctival hyperemia, follicular conjunctivitis) which generally resolve within 1 month of therapy.
This patient has done well, with no apparent side effects. It is my impression that topical interferon should the primary treatment for most cases of ocular surface squamous carcinoma and moderate to severe dysplasia.
Impression:
Topical Interferon Chemotherapy for Squamous Conjunctival Intraepithelial Neoplasia
References
Schechter BA, Schrier A, Nagler RS, Smith EF, Velazquez GE. Regression of Primary Conjunctival and Corneal Intraepithelial Neoplasia with Topical Interferon Alfa-2b. Cornea 2002; 21(1):6-11.
Wilson MW, Czechonska G, Finger PT, Rausen A, Hooper ME, Haik BG. Chemotherapy for eye cancer. Survey of Ophthalmology 45(5):416-444, 2001.
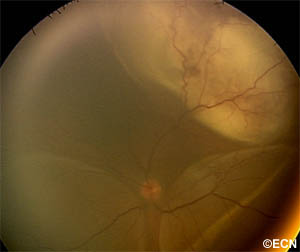
A RetCam digital image reveals an amelanotic subretinal tumor with intrinsic vascularity. Dependent exudative, bullous, nonrhegmatogenous retinal detachments are present in the inferior quadrants (Patient in supine position for RetCam). Image by Julian Garcia, MD
This 45 year old HIV positive patient was noted decreased vision in his left eye for 3 weeks duration. He had a past medical history of renal cell carcinoma with lung metastasis.
Impression
Choroidal Metastasis: of Renal Cell Carcinoma Origin
Treatment
This risks and benefits of chemotherapy and external beam radiation therapy were discussed in detail. Though he was to receive systemic chemotherapy, external beam irradiation was initiated due to the severity of his disease.
Comment
A RetCam digital image reveals an amelanotic subretinal tumor with intrinsic vascularity. Dependent Three-dimensional Ultrasound (3DUS) Image – This 3D reconstruction clearly demonstrates the variably reflective choroidal tumor as well as the secondary retinal detachment in the inferior quadrant.
This case presents multiple findings consistent with metastatic choroidal tumors: uveal mass and secondary retinal detachment. Multifocality and bilaterality can also be noted.
The presence of metastatic tumor in his lungs was a risk factor for uveal extension. All patients with intraocular metastasis should undergo radiographic imaging of their head, chest, and abdomen or total body PET/CT.
This case is unusual in that the most common primary cancers are breast in women and lung in men. Choroidal metastasis of renal cell origin are relatively rare.
In this case, our patient presented with a known primary cancer. Eighteen percent of patients will present with no known primary, most will have their primary discovered by subsequent systemic evaluations, and a few will have to undergo ocular fine-needle aspiration biopsy to help determine its source
Leukocoria with tumor visible through the right pupil. Note the clear cornea and lack of orbital signs.
This 16-month old patient was referred for bilateral leukocoria (white pupil), acute glaucoma OS, with evidence of anterior chamber seeding and possible optic nerve/orbital invasion. The left pupil was nonreactive.
Impression
Retinoblastoma
Note
This risks and benefits of observation, enucleation, chemotherapy and external beam radiation therapy were discussed in detail. Single agent cisplatinum chemotherapy (3 cycles due to definite choroidal and possible orbital and optic nerve involvement) and enucleation of the left eye was performed. Histopathologic evaluation of the left eye revealed retinoblastoma without optic nerve or orbital extension. The right eye was enucleated after failure of systemic chemoreduction to produce a treatable tumor.
Comment
This case presents multiple classic findings of retinoblastoma: leukocoria (white pupil), secondary glaucoma, orbital inflammation, anterior segment seeding, strabismus, and intraocular calcification. Other findings of retinoblastoma (not found in this case) can include pinealoma, and extraocular tumor extension. In North America today, when the tumor is confined to the eye more than 95% of children survive their retinoblastoma.
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.