One way to do that is providing as much information as possible before treatment even begins. The following video shows one couple’s perspective on home-care during ophthalmic plaque radiation therapy.
Plaque radiation therapy is the most widely used treatment for choroidal melanoma and delivers a highly concentrated radiation dose to the tumor. This treatment results in relatively less radiation to surrounding healthy tissues.
Rice-sized radioactive seeds are attached within a gold or steel bowl called a plaque. This is surgically implanted to the wall of the eye, covering the base of the intraocular tumor. After surgery, the patient is typically sent home for five to seven days while the low-energy radiation sterilizes the tumor.
Dr. Finger performed plaque radiation treatment on Stanley Fishman.
“When I was first diagnosed diffuse iris melanoma, it was a rather frightening and daunting experience. Fortunately, Dr. Finger was able to guide me through the process very calmly and in a low-key fashion throughout all of the subsequent treatments and recovery.”
Now you can benefit from Stanley’s experience in this video featuring him and his wife. It provides some valuable insight on what to expect during the treatment period and also offers great tips on how to manage home care during this time.
Researchers found using products to kill insects during pregnancy, and up to 1 month before, led to a 2.8-fold higher risk of nonhereditary, unilateral retinoblastoma in children.
Retinoblastoma is the most common intraocular childhood cancer. Each year it affects approximately 300 children in the United States and 8,000 worldwide. Even with cure rates of 99% in the developed world, 70% of children continue to die of retinoblastoma in less developed countries. There is a hereditary link in about 40% of cases. The risk factors for sporadic retinoblastoma remain largely unknown.
The results of this new study dovetail with a study published in 2013. Researchers found some indication of elevated retinoblastoma risk associated with paternal pesticide exposure in the workplace during the 10 years prior to conception.
The latest study focused on maternal exposure to pesticides. Researchers conducted detailed telephone interviews with the mothers of retinoblastoma patients. The study included 282 cases (186 unilateral and 96 bilateral) from the Children’s Oncology Group. Researchers analyzed retinoblastoma risk using healthy, age-matched controls.
The study found using both household pesticide products, such as Raid, and professional lawn or landscaping services, were similarly correlated with an elevated risk of retinoblastoma. Home weed killer products were also associated with higher risk, but the results were not statistically significant.
Dr. Renelle Pointdujour Lim analyzed the study.
“Analysis of combined parental exposures for both types of retinoblastoma (in one or two eyes) also suggests that the increased risk conveyed by pesticide use was similar among different types of pesticides, regardless of indoor or outdoor use, the time at which they were used during pregnancy, and whether it was the mother or father who applied them. However, these confidence intervals were also inconclusive.”
There were limits to the study. It used a relatively small sample size. There was also an issue with “recall bias,” because researchers had to rely on the memories of the subjects they interviewed. In general, “Retrospectively collected exposure data introduces the possibility of recall bias; therefore, results should be interpreted cautiously until additional studies are conducted,” researchers said.
While current research is far from conclusive, there is certainly enough evidence to raise red flags. It is reasonable to assume that parents should be careful about pesticide exposure during pregnancy, or if they are planning to get pregnant in the near future.
“I am sure pesticide use is the cause of many health problems. All of us should be more aware of what we introduce into our environment” said Dr. Paul Finger of The New York Eye Cancer Center.
There’s a new way to support the work of The Eye Cancer Foundation.
The ECF has partnered with Pledgeling, a platform that facilitates giving to nonprofits.
Visitors to pledgeling.com/home can search for specific non-profit organizations or general categories they want to support. For instance, searching for “eye cancer” will bring up The Eye Cancer Foundation. They can donate directly from that page.
But Pledgeling is more than just a stop on the Internet to drop off a donation. It is a fully integrated platform allowing businesses to support charitable giving.
Pledgeling’s goal is, “Powering the revolution for good.” The organization has helped to raise over $1 million for thousands of charities since its founding in 2014.
If you own a business, you can get involved and help support important ECF projects such as our 2020 Campaign to strategically train and place eye cancer specialists in unserved regions around the world.
Pledgeling works with Evite Donations to create a platform that allows you set up giving campaigns associated with your next party or function, thereby benefitting The Eye Cancer Foundation.
“The combination of Evite’s scale with Pledgeling’s charitable giving platform has made it possible to turn any face-to-face gathering into a moment of positive social impact,” Evite CEO Victor Cho said.
Pledgeling’s mobile-first technology platform and suite of software services will allow you to seamlessly incorporate a campaign to benefit The Eye Cancer Foundation into your business. This will not only help The ECF to create a world-class resource for eye cancer patients and their families, it will also help your business. As the folks at Pledgeling put it, “brands today must do good to do well.”
You can “do good,” by helping the mission of The Eye Cancer Foundation by utilizing Pledgeling to create a campaign.
For more information on how your business can partner with the ECF through Pledgeling, click here.
Comprehensive metastatic screening in patients diagnosed with choroidal melanoma is extremely important.
Patients at the New York Eye Cancer Center have access to all screening technology commercially available. For example, PET/CT screening was first investigated at NYECC. It is the only method that surveys the entire body for metastatic spread. In addition to an initial PET/CT scan, Dr. Paul Finger also customizes the use of subsequent MRI, CT, and ultrasound surveillance screening for his patients.
Unfortunately, many patients around only have access to the most basic metastatic screening. Many health services can only provide ultrasound screening. In some countries, there is no screening at all.
The American College of Radiology ranks both abdominal contrast enhanced MRI and CT as methods superior to ultrasound for detecting metastasis to the liver. Sadly, health care systems must weigh systemic costs against individual patient care. In contrast, patients just want the best diagnostic technologies and treatments available. At the New York Eye Cancer, patient-centered care means each individual patient’s needs come first. It’s all about excellence.
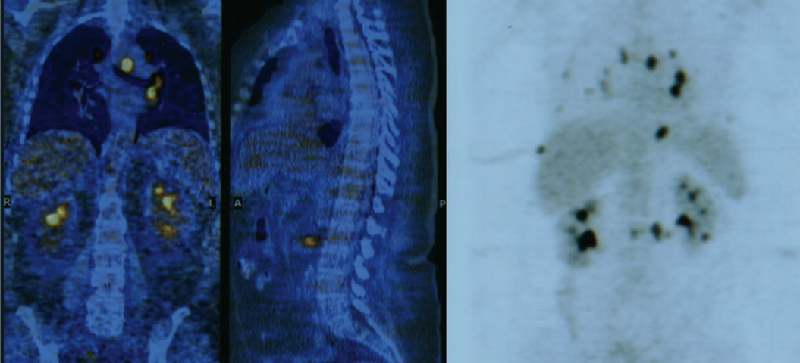
Pioneered by Dr. Finger at The New York Eye Cancer Center, ophthalmic total body 18 FDG PET/CT imaging combines two technologies to create a comprehensive screening process. In simple terms, CT imaging reveals the body’s anatomy (form). Positron emission tomography (PET) uses an acceptable amount of a radioactive sugar to reveal where tissues are active (function). A complex computer program puts the form and function images together to create a complete, anatomic, and metabolic 3D reconstruction of the patients body. PET/CT allows doctors to measure tumor size and shape, show its location and effect on normal anatomic structures, as well as its metabolically activity. By overlapping the metabolic and anatomic images, for the first time PET/CT puts form and function on the same diagnostic page.
While the liver is the most common place for choroidal melanoma metastasis, a study group led by Dr. Finger found that metastases can be found outside the liver (primarily bone and skin). Ultrasound screening focuses only on the liver misses these types of metastasis.
There are many factors that indicate increased risk for metastasis in choroidal melanoma patients. Based on these risk factors, individualized diagnosis, and the patients needs, Dr. Finger determines how to approach metastatic screening for each of his patients. Once the plan is in place, he has the best tools in the world at his disposal.
The theme of this year’s event is “We Can. I can.”
Cancer affects people in different ways, but everybody – together and as individuals – can take action to reduce the global burden of cancer.
The ‘We can. I can.’ campaign reinforces positive and action-oriented messaging about cancer. It also encourages the engagement of organizations and individuals in raising awareness and taking action against the disease.
On World Cancer Day, The Eye Cancer Foundation will join with groups and individuals around the world committed to fighting the scourge of cancer.
World Cancer Day is an important event to spread the word and raise cancer awareness around the globe. But more importantly, it’s a springboard for action.
In the coming year, The ECF will continue pushing forward with important projects related to diagnosing, treating, and ultimately curing eye cancer.
Retinoblastoma is a life and vision-threatening eye cancer that afflicts 10,000 young children every year. Our 2020 Campaign has committed to strategically train and place eye cancer specialists in underserved regions around the world. Our immediate goal is to save 1,000 young lives by the year 2020, but with the help of our generous donors, the sky is the limit.
This year, The ECF will host the Second Working Day on the first day of the International Society of Ocular Oncology meeting March 24 in Sydney, Australia. The Working Day will bring together eye cancer specialists from around the world to continue work on multicenter, international collaboration in ocular oncology.
Another important ECF initiative is the Eye Cancer Bioinformatics Grid (BIG). The mission of the BIG is to provide an infrastructure for sharing eye cancer data, results, and research. It is the first multicenter, international cooperative program focused on improving eye cancer research, diagnosis and patient care. Bio-informatics offers the chance for eye cancer specialists to work together and pool resources. As Eye Cancer Foundation Chairman Dr. Paul Finger says, “There is power in numbers.”
At The ECF, we are proud to do our part in the broader battle against cancer, and to join together with others around the world to celebrate World Cancer Day. We can. I can make a difference in the fight against cancer.
But all the technology in the world won’t help if patients never come in for an examination.
Eyelid, conjunctival, and corneal tumors are the easiest for patients to recognize. However intraocular and orbital tumors behind the eye are more difficult. Most patients with choroidal melanoma have no symptoms at all. These tumors are found by routine eye examinations, which highlight the need for everyone to periodically see their general ophthalmologist.
When symptoms do occur, it is crucial to know the signs and symptoms of eye cancers.
Flashes of light.
Squiggly lines, or floating objects.
Dark spot(s) on the iris.
Dark areas on the conjunctiva – the white of the eye.
Bulging or swelling of the eye or eyelid.
Pain in or around the eye.
Loss of eyelashes
Changes in the shape or size of the pupil.
White pupil.
Misdirection of the eye.
Excessive tearing or blood in the tears.
In children, a white spot can appear in the pupil known as“leukocoria.” This is best seen when light shines into the eye and is a common sign of retinoblastoma. This often shows up in flash photography.
Of course, these symptoms don’t necessarily mean you have eye cancer, but if you notice any of them, you should visit your eye doctor as soon as possible.
Remember that eye cancer often develops with no symptoms at all. This is why annual eye exams are crucial.
By knowing the signs and symptoms, getting regular eye exams, and acting quickly if any abnormalities appear, you can drastically increase your chances of catching eye cancer in its early stages.
Early, accurate diagnosis and prompt treatment can save both your vision and your life.
A new video offers a personal glimpse into the work of New York Eye Center Director Dr. Paul Finger.
Dr. Finger is an internationally recognized eye cancer specialist. He has spent 35 years in ophthalmic oncology, dedicating himself to learning, improving and inventing new methods for the diagnosis and treatment of cancers in and around the eye.
In addition to successfully treating thousands and thousands of patients, Dr. Finger has published more than 250 original articles, 38 book chapters, and has performed thousands of scientific reviews.
Reading about Dr. Finger’s work will give you a sense of his expertise and qualifications, but it simply doesn’t capture what truly drives him – concern for his patients.
That comes through in the video.
“What makes me happiest is that I come in every day, and I see patients who have been with me for 20 or 30 years, and most of them still see well from that eye.”
For more information about Dr. Finger and his work, Click Here.
A paper co-authored by Dr. Bikramjit P. Pal highlights a study conducted under the guidance of Dr. Tero Kivelä while supported by a fellowship grant provided by The Eye Cancer Foundation.
Dr. Pal worked under Dr. Kivelä at the Helsinki University Eye Hospital during a six-month fellowship from October 2015 through March 2016. During the fellowship, they conducted a study to follow the course of blood–brain barrier disruption maculopathy in a patient undergoing treatment for relapsed central nervous system lymphoma.
A primary central nervous system (CNS) lymphoma is a cancer inside the skull. Thankfully rare, CNS lymphomas account for about 3% of central nervous system cancers. Chemotherapy treatment is difficult due to the blood-brain barrier, a highly selective semipermeable membrane that separates circulating blood from the brain. Because many substances can’t pass through it, the blood-brain barrier protects the brain from most pathogens, but also limits the effectiveness of many chemotherapy agents.
A process called blood-brain barrier disruption (BBBD) can improve chemotherapy effectiveness in patients suffering from central nervous system lymphoma. The process involves the infusion of a warm hyperosmotic agent that allows the chemotherapy drugs to cross the barrier. BBBD results in a higher concentration of the drug by a factor of 50 to 100 times as compared with the standard intravenous route.
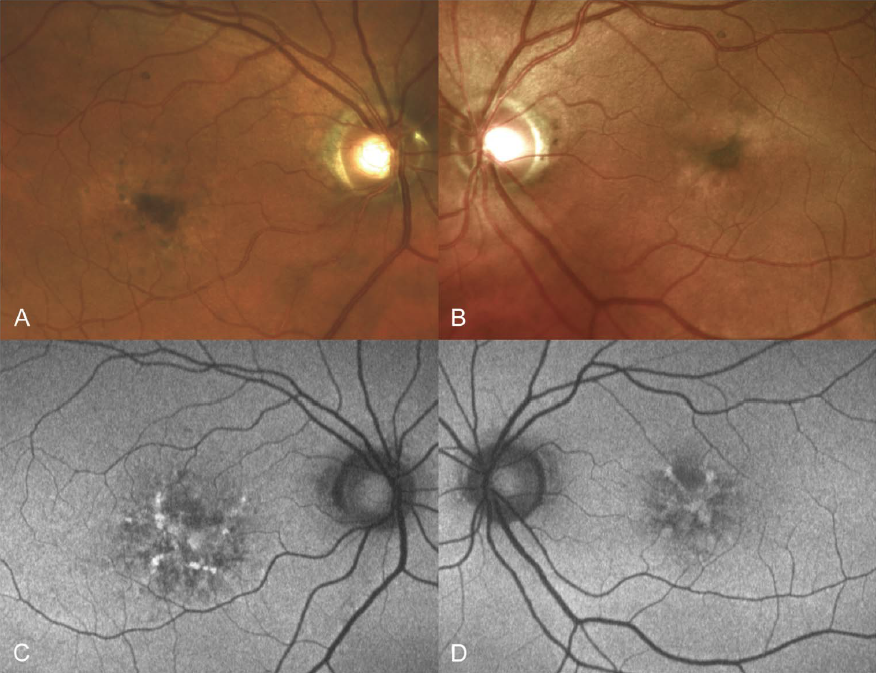
But there are risks involved in this BBBD-aided mode of treatment. Because the eye is part of the CNS and also shielded by the blood brain barrier, BBBD can cause a complication known as maculopathy. Maculopathy is damage to the macula (the functional center of the retina) resulting in a progressive loss of central vision. Mild to moderate loss of visual acuity (VA), and a nonprogressive nature, are the hallmarks of this condition in patients undergoing BBBD.
The study followed a 57-year-old patient diagnosed with central nervous system large B-cell lymphoma. He had a normal ophthalmic evaluation on his first visit. He was treated with blood–brain barrier disruption therapy and intra-arterial methotrexate. During the course of the therapy, he developed maculopathy with minimal eventual loss of visual acuity to 20/32 and 20/25 in his right and left eye respectively.
The study helped track the progression of maculopathy and provides some insight into the processes involved. It will certainly pave the way for further study.
“Although the maculopathy seems to be non-progressive and non-vision threatening, and the BBBD therapy usually is life saving as it was for our patient and cannot be abandoned, patients need regular follow-up as the full spectrum of this condition is probably not yet completely understood. Future studies incorporating fundus autofluorescence and OCT angiography may help in this regard.”
Dr. Tero Kivelä (left) with Dr. Bikramjit Pal in Siena, Italy. Dr. Pal was invited to Sienna to present research work he performed in Helsinki during his fellowship. This trip was supported by Dr. Doris Haudjistilianou.
Dr. Pal acknowledged the support of The Eye Cancer Foundation fellowship grant in the paper.
Dr. Pal plans to begin oncology services at a tertiary eye care facility in Kolkata. This center serves a huge population, not only in eastern India, but also in the neighboring countries of Nepal and Bangladesh.
Through its 2020 Campaign, The Eye Cancer Foundation plans to multiply this success story across the world. With your help, we can train 20 eye cancer specialists to work in 20 countries by 2020.
Our immediate 2020 Campaign goal is to save the lives of 1,000 children by 2020. But that’s only the beginning. Our ability to train doctors and supply them with the equipment they need to properly diagnose and treat retinoblastoma is only limited by the generosity of our donors.
You can become part of the cure with a one-time or recurring donation to The Eye Cancer Foundation. Click HERE to donate today.
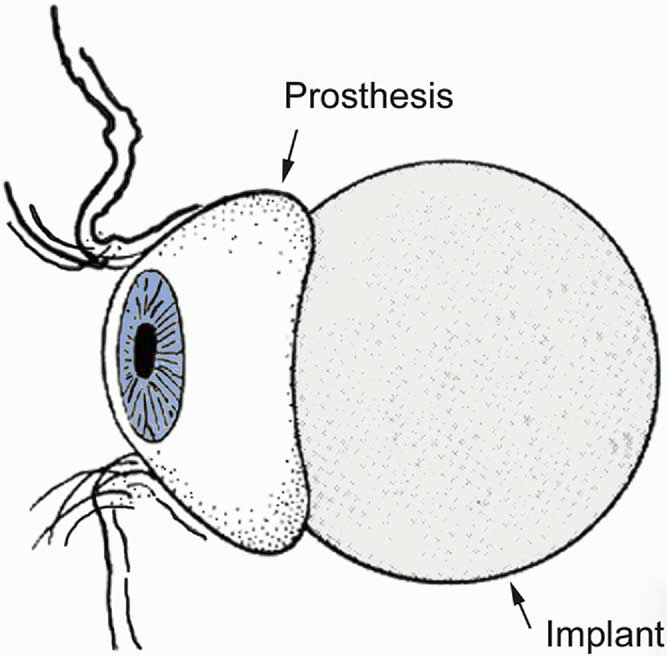
One of the most difficult aspects of losing an eye is psychological. For many patients, the first thing that pops into their mind is, “What will I look like.”
Fortunately, with a good ocular prosthesis, the loss of an eye will hardly be noticeable to the average passerby.
Over the last 20 years, the amount of time between surgery and the beginning of cosmetic rehabilitation has decreased from six weeks to typically less than four. In an effort to ease the psychological trauma of enucleation, Dr. Paul Finger has had great success reducing this timeframe even further. He has found most patients tolerate a temporary prosthesis in as little as five days. That means instead of waiting up to four weeks, they can have a temporary artificial eye inserted as soon as the bandage is removed. This greatly eases their psychological transition and facilitates a quick return to a sense of normalcy.
Dr. Finger co-authored a 2006 study published in Optometry – Journal of the American Optometric Association that showed patients generally did well with early insertion of a temporary prosthesis, and all of the study patients preferred the early cosmetic rehabilitation associated with placement of an ocular prosthesis at the time the bandage was removed.
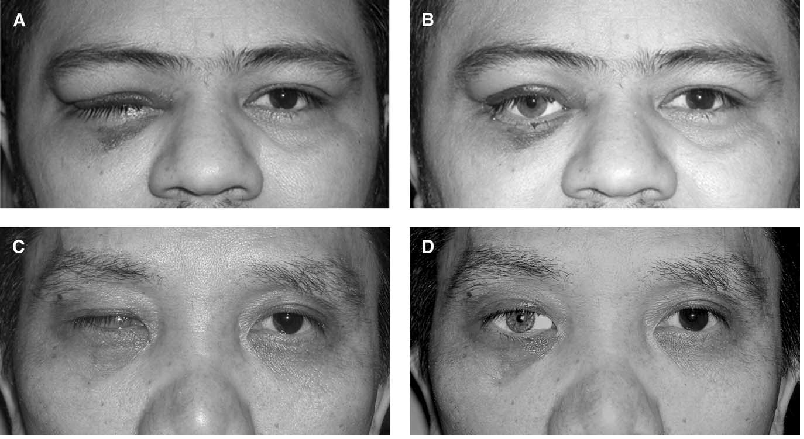
The study focused on 12 patients who had large intraocular malignancies and were treated by enucleation. Immediately after bandage removal, the patients saw themselves in a mirror and were offered placement of a relatively small ocular prosthesis. Patients were asked if they preferred their appearance with or without the prosthesis.
Eight patients tolerated introduction of the prosthesis at the time their pressure dressing was removed – three to five days after surgery. Due to discomfort, four patients did not receive their prostheses until their second postoperative visit – day 12 or 13. The manipulation at prosthesis insertion and subsequent wearing was found to have no effect on wound closure, final prosthetic fittings, or movement of the permanent prosthesis.
All of the patients preferred the appearance of the temporary prosthesis.
“Other than the temporary discomfort reported during four initial attempts at prosthesis insertion, there were no complications related to early cosmetic rehabilitation. There was no opening of the operative wound, infection, or hemorrhage. All patients were pleased with the cosmetic benefit afforded by early introduction of the prosthesis. They all made a stated preference for their appearance with the temporary prosthesis compared with their ‘pink eye’ with the conformer.”
Now, with 10 years of clinical experience supporting the study, almost every patient can be fitted with a temporary eye until their socket is ready for a permanent prosthetic solution.
The study underscores Dr. Finger’s commitment to patient centered care. This means not only treating the physical condition, but also considering the patient’s state of mind. The goal is not only to eradicate the cancer, but to help the patient to return to as normal and fulfilling life as possible.
Our primary goal is to find more effective ways to diagnose and treat eye cancer, but we also try to come up with innovations that make treatment more comfortable and less stressful for our patients.
Consider patients undergoing ophthalmic plaque radiation therapy. This course of treatment involves surgically implanting a radiation source onto the eye to cover the base of an intraocular tumor. The radiation sources used for brachytherapy come in the form of small “rice-sized” radioactive seeds. These seeds are attached within a gold or steel bowl called a plaque that is implanted on the eye. This process delivers a highly concentrated radiation dose to the tumor while exposing surrounding healthy tissue to relatively less radiation.
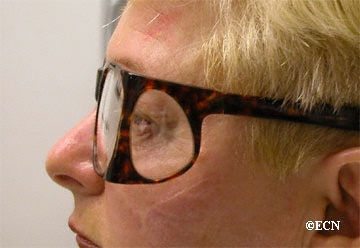
Patients undergoing plaque radiation therapy sometimes have to wear a lead patch over the eye to stop exiting radiation from entering into the environment. These opaque patches obscure vision in the affected eye for the duration of the treatment. This can last four to seven days.
This is particularly problematic for monocular patients with a tumor in their seeing eye. In this case, the lead patch will leave the patient blind during the course of their treatment. The patch can also create an uncomfortable inconvenience for patients who have vision in their untreated eye. They won’t be blind, but they will have to deal with diminished depth perception.
Dr. Paul Finger has come up with a simple yet innovative solution to this problem. He developed leaded glasses that effectively block exiting radiation while allowing patients with only one functioning eye to maintain their full vision throughout the treatment.
In a study funded by The Eye Cancer Foundation and published in the American Journal of Ophthalmology. Dr. Finger and Andrzej Szechter PhD found the leaded glasses improved patients’ quality of life without sacrificing radiation safety.
“Radiation-blocking glasses were remarkably helpful for our patients with only one functional eye. In these cases, use of the patch made them temporarily blind, disoriented, and dependent on others. Use of leaded safety glasses allowed these patients to see and function during ophthalmic plaque radiation therapy.”
This is a concrete example of what we call patient-centered care. The goal is not only to successfully treat the cancer, but to help the patient remain as comfortable as possible throughout the process.
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.