A new video offers a personal glimpse into the work of New York Eye Center Director Dr. Paul Finger.
Dr. Finger is an internationally recognized eye cancer specialist. He has spent 35 years in ophthalmic oncology, dedicating himself to learning, improving and inventing new methods for the diagnosis and treatment of cancers in and around the eye.
In addition to successfully treating thousands and thousands of patients, Dr. Finger has published more than 250 original articles, 38 book chapters, and has performed thousands of scientific reviews.
Reading about Dr. Finger’s work will give you a sense of his expertise and qualifications, but it simply doesn’t capture what truly drives him – concern for his patients.
That comes through in the video.
“What makes me happiest is that I come in every day, and I see patients who have been with me for 20 or 30 years, and most of them still see well from that eye.”
For more information about Dr. Finger and his work, Click Here.
A paper co-authored by Dr. Bikramjit P. Pal highlights a study conducted under the guidance of Dr. Tero Kivelä while supported by a fellowship grant provided by The Eye Cancer Foundation.
Dr. Pal worked under Dr. Kivelä at the Helsinki University Eye Hospital during a six-month fellowship from October 2015 through March 2016. During the fellowship, they conducted a study to follow the course of blood–brain barrier disruption maculopathy in a patient undergoing treatment for relapsed central nervous system lymphoma.
A primary central nervous system (CNS) lymphoma is a cancer inside the skull. Thankfully rare, CNS lymphomas account for about 3% of central nervous system cancers. Chemotherapy treatment is difficult due to the blood-brain barrier, a highly selective semipermeable membrane that separates circulating blood from the brain. Because many substances can’t pass through it, the blood-brain barrier protects the brain from most pathogens, but also limits the effectiveness of many chemotherapy agents.
A process called blood-brain barrier disruption (BBBD) can improve chemotherapy effectiveness in patients suffering from central nervous system lymphoma. The process involves the infusion of a warm hyperosmotic agent that allows the chemotherapy drugs to cross the barrier. BBBD results in a higher concentration of the drug by a factor of 50 to 100 times as compared with the standard intravenous route.
But there are risks involved in this BBBD-aided mode of treatment. Because the eye is part of the CNS and also shielded by the blood brain barrier, BBBD can cause a complication known as maculopathy. Maculopathy is damage to the macula (the functional center of the retina) resulting in a progressive loss of central vision. Mild to moderate loss of visual acuity (VA), and a nonprogressive nature, are the hallmarks of this condition in patients undergoing BBBD.
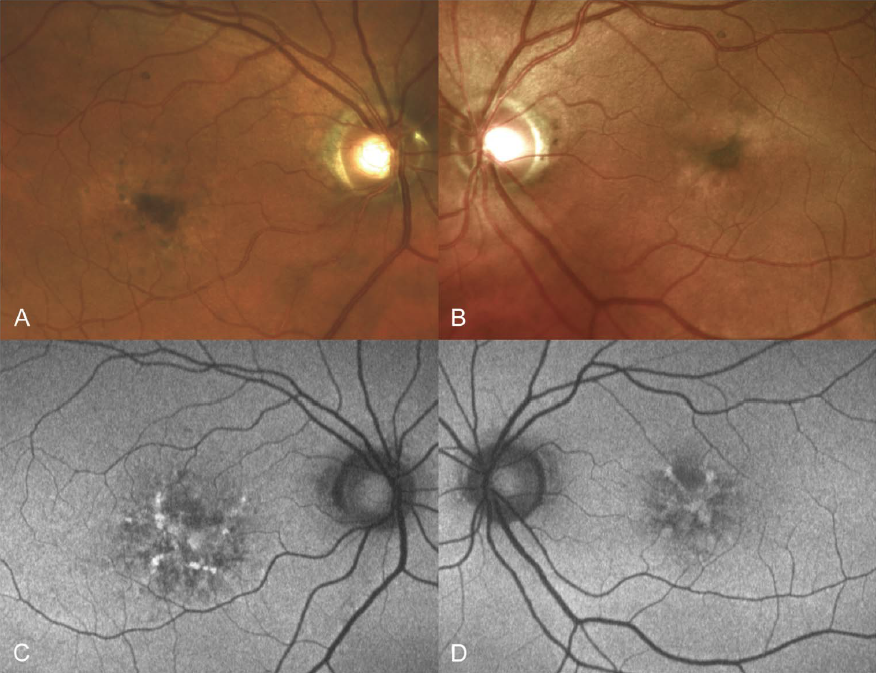
The study followed a 57-year-old patient diagnosed with central nervous system large B-cell lymphoma. He had a normal ophthalmic evaluation on his first visit. He was treated with blood–brain barrier disruption therapy and intra-arterial methotrexate. During the course of the therapy, he developed maculopathy with minimal eventual loss of visual acuity to 20/32 and 20/25 in his right and left eye respectively.
The study helped track the progression of maculopathy and provides some insight into the processes involved. It will certainly pave the way for further study.
“Although the maculopathy seems to be non-progressive and non-vision threatening, and the BBBD therapy usually is life saving as it was for our patient and cannot be abandoned, patients need regular follow-up as the full spectrum of this condition is probably not yet completely understood. Future studies incorporating fundus autofluorescence and OCT angiography may help in this regard.”
Dr. Tero Kivelä (left) with Dr. Bikramjit Pal in Siena, Italy. Dr. Pal was invited to Sienna to present research work he performed in Helsinki during his fellowship. This trip was supported by Dr. Doris Haudjistilianou.
Dr. Pal acknowledged the support of The Eye Cancer Foundation fellowship grant in the paper.
Dr. Pal plans to begin oncology services at a tertiary eye care facility in Kolkata. This center serves a huge population, not only in eastern India, but also in the neighboring countries of Nepal and Bangladesh.
Through its 2020 Campaign, The Eye Cancer Foundation plans to multiply this success story across the world. With your help, we can train 20 eye cancer specialists to work in 20 countries by 2020.
Our immediate 2020 Campaign goal is to save the lives of 1,000 children by 2020. But that’s only the beginning. Our ability to train doctors and supply them with the equipment they need to properly diagnose and treat retinoblastoma is only limited by the generosity of our donors.
You can become part of the cure with a one-time or recurring donation to The Eye Cancer Foundation. Click HERE to donate today.
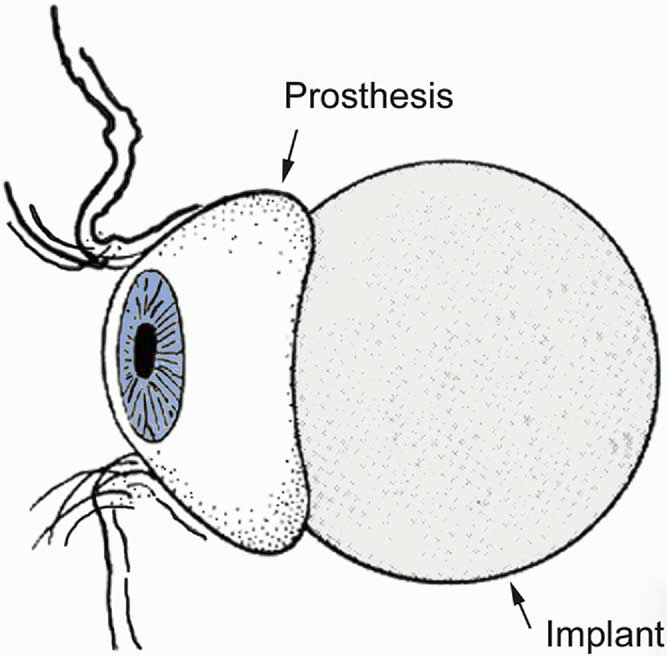
One of the most difficult aspects of losing an eye is psychological. For many patients, the first thing that pops into their mind is, “What will I look like.”
Fortunately, with a good ocular prosthesis, the loss of an eye will hardly be noticeable to the average passerby.
Over the last 20 years, the amount of time between surgery and the beginning of cosmetic rehabilitation has decreased from six weeks to typically less than four. In an effort to ease the psychological trauma of enucleation, Dr. Paul Finger has had great success reducing this timeframe even further. He has found most patients tolerate a temporary prosthesis in as little as five days. That means instead of waiting up to four weeks, they can have a temporary artificial eye inserted as soon as the bandage is removed. This greatly eases their psychological transition and facilitates a quick return to a sense of normalcy.
Dr. Finger co-authored a 2006 study published in Optometry – Journal of the American Optometric Association that showed patients generally did well with early insertion of a temporary prosthesis, and all of the study patients preferred the early cosmetic rehabilitation associated with placement of an ocular prosthesis at the time the bandage was removed.
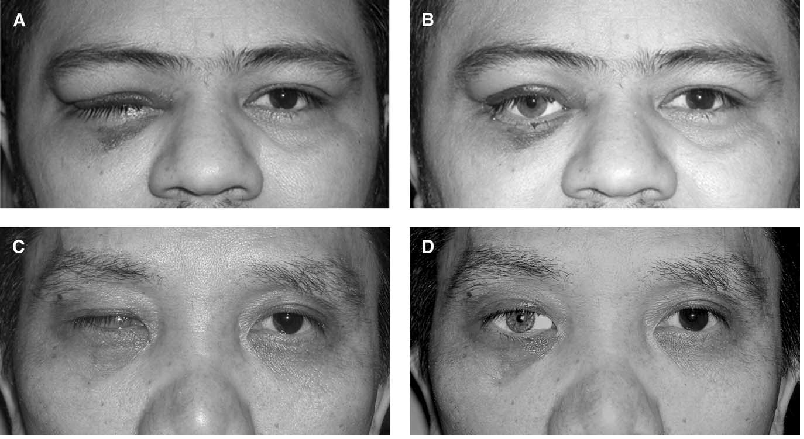
The study focused on 12 patients who had large intraocular malignancies and were treated by enucleation. Immediately after bandage removal, the patients saw themselves in a mirror and were offered placement of a relatively small ocular prosthesis. Patients were asked if they preferred their appearance with or without the prosthesis.
Eight patients tolerated introduction of the prosthesis at the time their pressure dressing was removed – three to five days after surgery. Due to discomfort, four patients did not receive their prostheses until their second postoperative visit – day 12 or 13. The manipulation at prosthesis insertion and subsequent wearing was found to have no effect on wound closure, final prosthetic fittings, or movement of the permanent prosthesis.
All of the patients preferred the appearance of the temporary prosthesis.
“Other than the temporary discomfort reported during four initial attempts at prosthesis insertion, there were no complications related to early cosmetic rehabilitation. There was no opening of the operative wound, infection, or hemorrhage. All patients were pleased with the cosmetic benefit afforded by early introduction of the prosthesis. They all made a stated preference for their appearance with the temporary prosthesis compared with their ‘pink eye’ with the conformer.”
Now, with 10 years of clinical experience supporting the study, almost every patient can be fitted with a temporary eye until their socket is ready for a permanent prosthetic solution.
The study underscores Dr. Finger’s commitment to patient centered care. This means not only treating the physical condition, but also considering the patient’s state of mind. The goal is not only to eradicate the cancer, but to help the patient to return to as normal and fulfilling life as possible.
Our primary goal is to find more effective ways to diagnose and treat eye cancer, but we also try to come up with innovations that make treatment more comfortable and less stressful for our patients.
Consider patients undergoing ophthalmic plaque radiation therapy. This course of treatment involves surgically implanting a radiation source onto the eye to cover the base of an intraocular tumor. The radiation sources used for brachytherapy come in the form of small “rice-sized” radioactive seeds. These seeds are attached within a gold or steel bowl called a plaque that is implanted on the eye. This process delivers a highly concentrated radiation dose to the tumor while exposing surrounding healthy tissue to relatively less radiation.
Patients undergoing plaque radiation therapy sometimes have to wear a lead patch over the eye to stop exiting radiation from entering into the environment. These opaque patches obscure vision in the affected eye for the duration of the treatment. This can last four to seven days.
This is particularly problematic for monocular patients with a tumor in their seeing eye. In this case, the lead patch will leave the patient blind during the course of their treatment. The patch can also create an uncomfortable inconvenience for patients who have vision in their untreated eye. They won’t be blind, but they will have to deal with diminished depth perception.
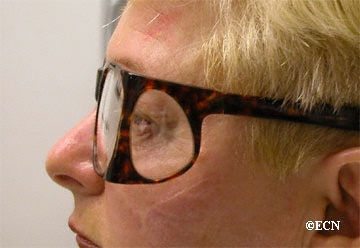
Dr. Paul Finger has come up with a simple yet innovative solution to this problem. He developed leaded glasses that effectively block exiting radiation while allowing patients with only one functioning eye to maintain their full vision throughout the treatment.
In a study funded by The Eye Cancer Foundation and published in the American Journal of Ophthalmology. Dr. Finger and Andrzej Szechter PhD found the leaded glasses improved patients’ quality of life without sacrificing radiation safety.
“Radiation-blocking glasses were remarkably helpful for our patients with only one functional eye. In these cases, use of the patch made them temporarily blind, disoriented, and dependent on others. Use of leaded safety glasses allowed these patients to see and function during ophthalmic plaque radiation therapy.”
This is a concrete example of what we call patient-centered care. The goal is not only to successfully treat the cancer, but to help the patient remain as comfortable as possible throughout the process.
In fact, you may actually need those sunglasses more in the winter than during the summer.
In the summertime, most of us instinctively reach for the sunglasses as we walk out the door. But during the winter, it’s easy to leave them sitting on the table. After all, it’s not usually terribly bright out, even on sunny days, and oftentimes it’s gloomy and overcast.
During the winter months, the sun sits lower in the sky, changing the angle. It seems less bright, but this can actually increase your exposure to dangerous UV rays, according to Jessica Lattman, a board-certified ophthalmologist. The risk increases when snow covers the ground. Scientists say snow reflects up to 85 percent of the sun’s UV rays. It’s so intense, it can actually sunburn your corneas.
Skiers need to be especially vigilant.
“UV radiation increases 5% for every 1,000 feet you go above sea level,” Lattman told the Huffington Post. “When you are skiing or outside at higher elevations, the exposure is even greater. At 5,000 feet, you will be exposed to 20% more radiation from the sun.”
That’s why it’s imperative to wear skiing goggles that block UV rays.
Your winter eyewear should meet the same standards as the sunglasses you wear in the summer. It should block all UVA, UVB, and UVC rays. You want to make sure the glasses provide 100% UV protection. Many optical shops have a machine called a photometer that measures UV transmission through glasses. You want to wear sunglasses or goggles that block all UV radiation or light under 400 nm in wavelength.
So, when you run out the door this winter, don’t forget to grab those sunglasses – sunblock for your eyes.
Dealing with the loss of an eye can make patients feel conspicuous and awkward. Darrell Hardin has just the prescription – compassion, humor and beautiful artificial eyes.
Hardin is an ocularist in Willoughby, Ohio. He combines technical skill with a sense of artistry to make eyes for patients who have lost them due to disease or injury. He offers hope for a sense of normalcy for his patients by creating realistic artificial eyes. But he does much more for those who walk into his office, as a recent story in the Cleveland Plain Dealer describes
“Hardin’s irreverent, sometimes corny, sense of humor serves to put patients at ease, and to let them know that it is OK, healing, even, to laugh at the circumstances that caused them to seek his services.”
As the saying goes, sometimes laughter is the best medicine.
Losing an eye is traumatic. Patients can experience a profound sense of loss, depression and self-consciousness about how they look. Hardin’s demeanor helps lift the gloom.
He has a particular empathy for cancer patients. He battled the disease himself.
“Hodgkins in the ’70’s,” he told the Plain Dealer. “I know . . . I thought, ‘Oh, I’m gonna die.’ But my 87-year-old aunt says ‘God doesn’t want a weed in his garden, and the Devil doesn’t want competition.’”
Hardin can also intimately empathize with patients who have lost an eye. His wife Cindy was born with glaucoma and had an eye removed in her 30s.
“If my wife had both eyes, she probably wouldn’t be with me.” He laughs and then turns more serious. “I finally found a person who understands what I do, and why.”
Hardin calls his work his passion. He paints each eye by hand, creating a prosthetic that is hardly noticeable to the average passerby. It is now possible to produce artificial eyes digitally, but Hardin says they don’t have the depth of hand-painted prosthetics.
“It’s not an ego trip. I try to do my best. My goal is for you not to notice my work.”
Hardin’s work underscores two important points.
First, even if you lose an eye, it’s possible to live a normal life. Most patients can see with their remaining eye and will most likely be able to do all the things they used to do before, even drive a car. With modern eye prosthesis, the loss of the eye is hardly noticeable, as you can see in our enucleation after-image gallery.
Second, a human touch is vital when interacting with people facing adversity such as the loss of an eye, or a diagnosis of eye cancer. At the New York Eye Center, we call this “patient-centered care,” and it’s the foundation of everything we do.
Photo Credit: Wellcome Library, London. Used under creative common license
The Eye Cancer Foundation publishes The Visionary free-of-charge to keep you informed about the latest news, research, and global efforts focused on improving eye cancer treatment, diagnosis, and cure.
In this edition, you will find articles about:
Projects for the second Eye Cancer Working Day
The 2020 Campaign to save the lives of 1,000 children by 2020
Lost Eye: A networking community for enulceated patients
Early screening for retinoblastoma in infants is key to saving vision and life.
Retinoblastoma is the most common intraocular childhood cancer. It affects approximately 300 children in the United States each year and more than 8,000 worldwide. When detected early, the cure rate is high. But if the diagnosis is delayed, it can result in the loss of an eye and even death.
In all cases, early screening is important to detect cancer in its beginning stages. Doctors should regularly examine the child’s eyes, and parents should be aware retinoblastoma symptoms. White spots appearing when light shines into the eye is the most common sign. This often shows up in flash photography. Other symptoms include a lazy eye, vision problems, redness in the white part of the eye, bulging eyes, changes in the color of the iris, and unequally reactive pupils.
The importance of screening is magnified in children with a family history of retinoblastoma. They need to be examined by an ophthalmologist immediately after birth. Regular examinations should be continued for the next 5 to 6 years, at least once every 3 to 6 months.
Genetic testing is another option for children with a family history of retinoblastoma.
“Genetic testing is so important in retinoblastoma, the American Joint Committee on Cancer RB-Section headed by Ashwin Mallipatna MD achieved approval for heredity to be included in the 8th edition AJCC RB Cancer Staging System,” notes Dr. Paul T. Finger, Chair of The AJCC Ophthalmic Oncology Task Force.
In India, the Orbit and Oculoplasty Clinic of Aravind Eye Hospital recently opened its Ocular Cancer Genetic Centre. India has the highest incidence of retinoblastoma in the developing world. According to an article in the Journal for Human Genetics, about 40% of Indian patients suffer from the hereditary form of RB.
“After providing treatment, prosthetic eye and rehabilitation for patients for years, the question of what we could do to prevent RB kept haunting us. If we are able to see the tumor early, we can save the life of the child. But if we find out the predisposition to RB from gene mutation in either of the parents, we can save both vision and life of the child,” Usha Kim, chief, Orbit, Oculoplasty and Oncology Clinic, told The Hindu.
Mutations in the RB1 gene are responsible for hereditary retinoblastoma. Due to the gene’s large size and complexity, genetic testing can be cumbersome. To overcome the problem, researchers in India developed a rapid screening strategy by prioritizing sections of the DNA.
“Using this strategy for genetic analysis, mutations were identified in 76% of patients in half the actual time and one third of the cost. This reduction in time and cost will allow for better risk prediction for siblings and offspring, thereby facilitating genetic counseling for families, especially in developing countries.”
Advances in genetic testing will make screening more widely available, especially in developing countries. Children with family histories of retinoblastoma should undergo genetic screening when possible. But nothing can replace diligent doctors and parents being aware of the symptoms, and making sure children get regular eye examinations.
Patient Stories
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.