Malignant tumors from other parts of the body can spread into and around the eye. Though they are the most common intraocular cancer in adults, they usually go undetected. This is because most ocular metastases go undetected unless they affect vision, are visible to the patient, or push the eye forward. Eye metastasis are most commonly found in the vascular choroid (choroidal metastasis) within the eye.
Ocular or eye metastasis are usually from a breast cancer (in women) and lung cancer (in men). Other less common sites of origin include the prostate, the kidney, the thyroid, and gastrointestinal tract. Blood cell cancer (lymphoma and leukemia) can also metastasize into the eye and orbit. In 18% of patients, the primary source of the metastasis may be undetectable. In these cases, Dr. Finger may have to biopsy the ocular tumor to obtain tissue for pathology (to determine the primary source).
Symptoms
As stated, most patients with choroidal metastasis have no symptoms. However, if the metastasis is on the eye or eyelids, it may be visible. If the metastasis is located behind the eye (in the orbit), the eyeball may be visibly displaced out or to the side. If the metastasis is within the eye (the most common), metastasis patients can can have symptoms of flashing lights, floating spots or distortion of their vision. In that waiting until patients are symptomatic may be too late to preserve vision, Dr. Finger suggests that all patients with a history of metastatic cancer should have periodic eye examinations.
Diagnosis
In that most patients with ocular metastasis have either a known primary cancer and/or metastatic tumors in other parts of their body; a careful medical history is important. Patients know of prior cancer history and many can remember their tumor stage. History taking can also uncover the signs or symptoms of these other cancers. If an eye cancer specialist suspects ocular metastasis, both eyes and orbits should be examined because ocular metastases can be both bilateral and/or multifocal.
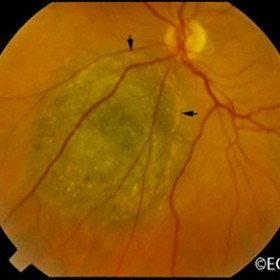
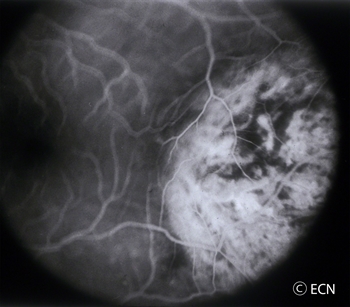
Choroidal metastasis is usually non-pigmented (except metastatic melanomas), and has typical ultrasound and angiographic patterns. Choroidal metastasis is usually poorly circumscribed and can cause retinal detachments. They may have spicules of pigment on their surface. Fluorescein angiography may reveal a typical, “starry sky” of hyper-fluorescent micro-aneurysms. Unlike primary choroidal melanoma, they can grow quickly (weeks) and may require prompt treatment.
The patient with metastasis to the eye should also be examined by a medical oncologist. A complete metastatic survey should be performed to “stage” the patient (to see if there are other tumors within the body). Specifically, radiographic imaging including but not necessarily limited to the brain and lung should be performed due to a high concurrent incidence of intracranial and pulmonary metastases. Dr. Finger will likely suggest a total body PET/CT with fusion.
Treatments
After irradiation, a regressed choroidal metastasis displays spicular hypertrophy of the retinal pigment epithelium.
Most patients with ocular metastasis have either a known primary cancer and/or metastatic tumors in other parts of their body. A careful medical history can uncover the signs or symptoms of these other cancers. If an eye cancer specialist suspects ocular metastasis, both eyes and orbits should be examined because ocular metastases are commonly both bilateral and/or multifocal.a
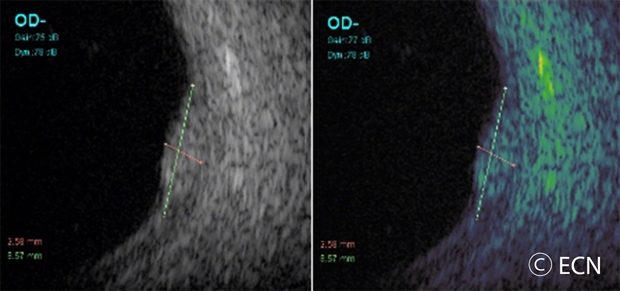
Choroidal metastasis are usually non-pigmented, yellow or white (except metastatic melanomas). Choroidal metastasis is usually poorly circumscribed and can cause retinal detachments. They may have spicules of pigment on their surface. Unlike primary choroidal melanoma, they can grow quickly (weeks) and may require prompt treatment. They typically have typical ultrasound findings of variable reflectivity, angiographic (starry sky microaneurysm) and OCT wavy surface patterns that are helpful to establish the diagnosis.
Treatment depends on the type of metastasis and its primary source. Treatment options often include chemotherapy, immunotherapy and radiation therapy. In general, chemotherapy and immunotherapy take a relatively long time to work, whereas radiation therapy is more rapid. The choice of chemotherapy, immunotherapy or radiation therapy typically depends on the type of tumor and the temporal “timing” risk for loss of vision.
FAQs
Q: If I have been diagnosed with cancer, and have no symptoms should I get my eye checked? A: It is reasonable to have a yearly-dilated eye examination (with examination of your retina).
Q: If I am on chemotherapy do I need to have radiation too? A: If chemotherapy is controlling your eye tumor you may not need additional radiation therapy.
Q: If I have a metastatic cancer in one eye, can another occur in my other eye? A: Yes, you should be monitored every 3 to 4 months.
Tumors of the eyelids may be benign cysts, inflammations (styes), or malignant tumors (skin cancers). The most common type of eyelid cancer is basal cell carcinoma. Most basal cell carcinomas can be removed with surgery. If left untreated, these tumors can grow around the eye and into the orbit, sinuses and brain. Other eyelid cancers include squamous cell carcinoma, sebaceous cell carcinoma, and malignant melanoma. Together, these tumors make up the remaining 10% of eyelid malignancies.
Symptoms
Most patients with eyelid tumors will notice a nodular growth on their eyelid. This growth can be skin colored, red, brown or black. Malignant tumors may cause loss of eyelashes or distort the position of the eyelid. All patients with eyelid tumors should be evaluated by an eye care specialist with experience in the care of eyelid tumors.
Diagnosis
A simple biopsy can determine if an eyelid tumor is malignant.
Treatments
Malignant tumors are completely removed and the eyelid is repaired using plastic surgery techniques. Some doctors are now using topical immunotherapy or chemotherapy agents to avoid surgery. Dr. Finger can sometime use “Finger-tip” cryotherapy (freezing-therapy) or radiation therapy, depending on the extent of the tumor.
Additional info
A Typical Work-up for a Suspected Malignant Eyelid Tumor:
General: The goal should be total removal of the eyelid cancer. This usually involves primary excision with either frozen section control or the Moh’s technique.
Small tumors are usually removed by pentagonal wedge resection.
Medium-sized tumors often require reconstruction with transpositional flaps (Tenzel, Mustarde, Glabellar).
Large-tumor resections are typically reconstructed with Hughes, Hewes or Cutler-Beard Techniques.
The wall of the eye has 3 main layers. From outside to inside there is: the white sclera, a blood vessel layer called the uvea (choroid, ciliary body and iris) and an inner retinal layer. Further, the pigment producing cells, “melanocytes” are primarily found in the vascular uveal layer. It is those melanocytes that can turn into malignant melanoma. Therefore, when melanoma happens in the choroid, they are called “choroidal melanoma,” the most common primary intraocular malignancy in adults. That said, choroidal melanomas are rare with 5 to10 out of each million people diagnosed with a choroidal melanoma each year. Choroidal melanomas can spread to other parts of the body.
Eye cancer specialists can determine if you have a choroidal melanoma by performing a complete eye examination with testing. This includes asking questions about your medical history, examining both of your eyes, looking into the eye through a dilated pupil, performing an ultrasound examination, and specialized photography (to examine the circulation within the choroidal melanoma).
MOST – Fingers’ Melanoma Mnemonic
Dr. Finger has developed the mnemonic device “MOST” to help eye care specialists to determine if the intraocular tumor is a melanoma.
“M,” Melanoma:
“O,” Orange Pigment Lipofuscin (OPL) a metabolic side product of cell death. This finding tells us that that either the underlying tumor is destroying the overlying tissue or itself is degenerating. Lipofuscin is best seen with a photographic test called Fundus Auto Fluorescence imaging, or FAF.
“S,” Subretinal fluid (SRF) is created by poorly formed or new, “neovascular” blood vessels within the tumor. Cancers need new vessels in order to grow. Large amounts of SRF can be seen by ophthalmoscopy (looking into the eye) and ultrasound imaging. However, small amounts of SRF are best seen on 3D optical coherence tomographic imaging (3D-OCT).
“T,” Thickness of the tumor has been associated with malignancy. Simply, the thicker it is the more likely a pigmented intraocular tumor is malignant. It is widely accepted that tumors greater than 2.0 mm are more likely to be malignant. Ultrasound imaging is currently the best method to measure tumor thickness.
Your specialist will also request that you have a complete general medical check up and specific tests depending upon what they see inside your eye. In the Collaborative Ocular Melanoma Study (COMS), participating eye cancer specialists correctly diagnosed select choroidal melanoma in over 99.6% of cases (without a biopsy). That said, patients with unusual appearing “atypical” tumors were not entered into the study.
Classic Indications for Biopsy
Atypical tumor, metastatic tumor with no observable primary cancer and when the patient requests a pathology diagnosis. More recently, primarily due to genetic testing services, more and more centers are routinely performing choroidal tumor biopsy primarily for genetic tumor analysis. Genetics offers information about the tumor, but does not allow doctors to avoid treatment or follow up systemic testing for metastasis.
Choroidal biopsy has been associated with a risk of hemorrhage, infection, retinal detachment and a poorly quantified risk of tumor seeding (outside the eye). Risks related to tumor seeding are thought to be small, but clearly they have not been evaluated by any large prospective or retrospective study. Each eye cancer specialist should discuss the relative risks (known and unknown) of biopsy prior to surgery.
Questions About Intraocular Biopsy:
Remove the need for surgical tumor treatment?
Reduce the number of radiologic examination or years needed for systemic surveillance?
What are the risks of biopsy (hemorrhage (e.g. vitreous, subretinal, subfoveal), seeding, damage to the lens, optic nerve, retinal detachment, cataract, epiretinal membrane, loss of vision, loss of eye and/or reaction to anesthesia).
Symptoms
Most choroidal melanoma patients have no symptoms. The melanoma is found on routine eye examination. If patients have choroidal melanoma symptoms, they are usually seeing “flashes of light,” noticing “distortion” or loss of vision, and floating objects (floaters) in their vision.
If the choroidal melanoma is in the front of the eye (near the natural lens), it can push or tilt the natural lens causing an irregular astigmatism (blurring of vision).
Choroidal melanoma can leak fluid beneath the retina, making the retina detach and cause symptoms of flashing lights and floating specks “floaters”.
If the choroidal melanoma is in the macula (center of vision), it can grow beneath the fovea making the patient far-sighted. The choroidal melanoma can also grow into and destroy the fovea causing distortion, loss of vision or changes in color perception.
It is important to note that most patients with choroidal melanoma have no symptoms at all. Their tumors are found when they visit their eye doctor for a “routine” eye examination. So everyone should have periodic eye examinations (including dilated ophthalmoscopy). In general, the earlier and smaller the choroidal melanoma, the better the prognosis for both life and sight.
Other, more unusual presentations of anterior choroidal and iridociliary melanoma are discoloration of the iris, a brown spot on the outside of the eye, an irregularly shaped pupil and glaucoma.
Diagnosis
Choroidal melanoma is usually seen by ophthalmoscopy (when your eye doctor looks through a lens into your dilated pupil). Choroidal melanoma has typical “diagnostic” characteristics that include but are not limited to: pigmentation, low to moderate internal ultrasound reflectivity, clumps of orange pigment lipofuscin on its surface, leakage of subretinal fluid, or retinal detachment (on or around the choroidal melanoma) and thickness.
Pigmentation is due to naturally occurring melanin that comes from melanocyte cells in the choroidal layer of the eye. Choroidal melanomas are most commonly pigmented, but can be variably pigmented and even non-pigmented (amelanotic). Non-pigmented choroidal melanoma is due to a proliferation of melanocytes that have lost their ability to make the melanin pigment.
Orange pigment is made up of a chemical called lipofuscin and appears on the surface of choroidal melanomas. Lipofuscin is a product of cell death which indicate that cells are dying on the tumor’s surface. This is also sign of metabolic activity. Melanomas are more metabolically active than choroidal nevi.
Ultrasound is typically used to measure the choroidal melanoma size, evaluate internal tumor reflectivity, and look for melanoma extension behind the eye into the orbit called extrascleral extension. Ultrasound imaging has demonstrated that most choroidal melanomas are shaped like a dome and less commonly like a mushroom. Ultrasound can also evaluate and detect choroidal melanoma associated retinal detachment. However, optical coherence tomography (OCT) is a more sensitive way to detect subretinal fluid – retinal detachment.
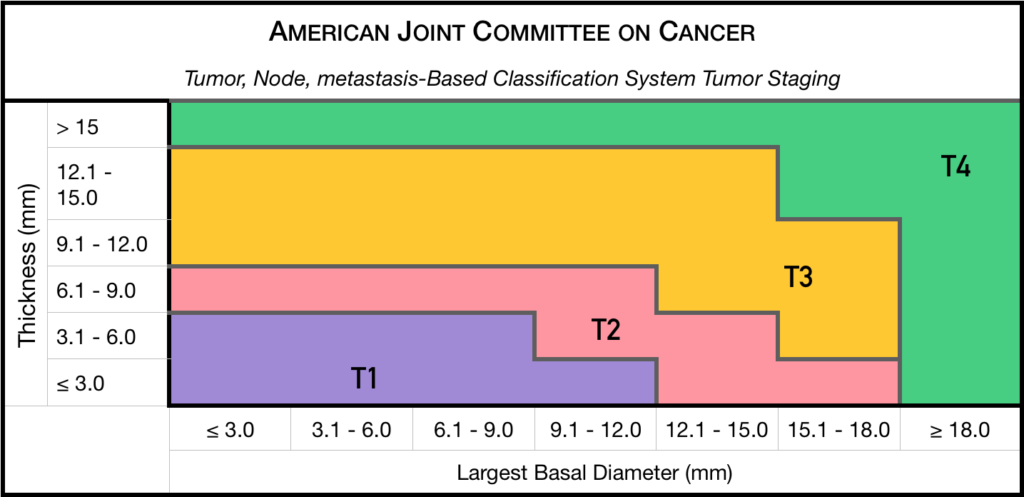
Staging
Chaired by Dr. Paul T. Finger, a committee of top ophthalmic specialists assembled to form the AJCC-UICC Ophthalmic Oncology Task Force. To ensure a broad range of specialists, Dr. Finger “internationalized” the committee, including over 58 members both from the USA and around the world.
This committee had one driving goal: to design a clinically useful Tumor-Node-Metastasis (TNM) based classification “language” for ocular tumors. This first-of-its-kind classification system has become a universal language for all who diagnose and treat ocular tumors.
Not only does a universal classification system offer cancer staging for the patient, it also allows physicians to directly compare data. In the long run, a common “eye tumor” language helps usdetermine and differentiate treatment types as well as coordinate the efforts of researchers working for a cure.
Dr. Finger has since translated this staging system for the worlds’ Union International for Cancer Control (UICC), and offered it to the world. In order to get everyone to employ this new language, he has recruited all the major medical journals to require eye cancer researchers to use AJCC-UICC staging.
Treatments
Small Choroidal Melanoma (AJCC T1 and T2): Patients with a small choroidal melanoma can be treated after their first visit, but since growth helps to prove that the tumor is a cancer, your doctor may suggest “observation” or watching for a small amount of choroidal melanoma growth prior to treatment. Your eye cancer specialist should discuss the relative risks and potential benefits of “observation for growth” as compared to “immediate treatment” for choroidal melanoma. If growth is documented (typically within 6 months of observation), eye cancer specialists will typically recommend definitive treatment.
Medium-sized Choroidal Melanoma (AJCC T3 and T4): Most patients with large-sized choroidal melanoma can be also be treated with eye-sparing low energy radiation therapy (e.g. palladium-103). However, larger tumors require more radiation and larger irradiated intraocular volumes resulting in greater risk of radiation side-effects and poor vision. Rarely such eyes have to be secondarily removed. Eye cancer specialists try to preserve eyes, even if the eye had reduced vision.
Large-sized Choroidal Melanoma: Very large choroidal melanomas (greater than 22 mm width) may be treated by initial removal of the eye (enucleation). This is because the amount of radiation required to destroy a choroidal melanoma that fills most of the eye will likely be too much for the eye to tolerate.
However, most patients, even with very large-sized choroidal melanoma can be treated with eye-sparing radiation therapy. However, after eye sparing radiation for very large choroidal melanomas, eyes are at greater risk to have poor vision, secondary inflammation and may require secondary removal at a later date.
Additional Info
Patients often ask why they have a choroidal melanoma. While there is no one cause, choroidal melanoma is more common among patients with blue vs. brown eyes, those with outdoor occupations, and in Australia where there is a hole in the ozone layer. Therefore, though this hypothesis has yet to be proven, it seems reasonable to assume that choroidal melanoma is related to sunlight (ultraviolet exposure).
In that sunlight exposure has been linked to several eye cancers and diseases of the eye, Dr. Finger suggests that you “Think of Sunglasses as Sun Block for your Eyes” ™ and start wearing your UV blocking sunglasses. They make great gifts too!
Dr. Finger also often gets questions related to stage and spread. These two things are closely linked––choroidal melanoma size is most closely related to its risk for spread to other parts of the body (metastasis). In three separate studies, cumulatively involving almost 20,000 patients, the average rate of metastasis has been 50%. However, patients with smaller tumors have much lower rates compared to larger tumors. Therefore, patients should ask their eye cancer specialist about their tumors AJCC-UICC tumor size and risk for metastasis. In general, the larger the choroidal melanoma the worse the prognosis for both vision and metastasis.
Hemangiomas can grow within the blood vessel layer beneath the retina called the choroid. If they are located in the macula (center of vision) or they leak fluid (which causes a retinal detachment or cystic changes in the retina), they can affect visual acuity. However, many choroidal hemangiomas never grow or leak fluid and can be observed without treatment. Choroidal hemangiomas are not cancers and never metastasize.
Symptoms
<justify?This choroidal hemangioma lies above the optic nerve, but extends into the fovea. Though there was no serous detachment, cystoid retinal degeneration of the fovea caused decreased visual acuity to 20/200.
On your left, there is a red colored choroidal hemangioma just above the round optic nerve. Typically, choroidal hemangioma are reddish to orange colored. They can have areas of increased pigmentation which can make them difficult to differentiate from choroidal melanomas.
By lifting the overlying retina, choroidal hemangiomas can cause far-sightedness (hyperopia), distorted vision (metamorphopsia), flashing lights, or blurred vision. Choroidal hemangioma that cause no symptoms at all, are usually found on routine dilated eye examinations (ophthalmoscopy).
Diagnosis
Course Vascular Pattern
Intraocular Photography and Angiography: An eye care specialist can perform studies of the blood flow within the eye by injecting drugs called fluorescein or indocyanine green. They can also look at the overlying blood vessels with computerized optical coherence tomography – angiograpy (OCT-A). When drugs are injected into the arm or hand, they will travel into the blood vessels inside the eye. Using special lights that make the angiographic dyes fluoresce, your doctor can see special differentiating circulation patterns, that help differentiate between the types of tumors. For example,choroidal hemangioma have a unique pattern of circulation where the large blood vessels produce a “COARSE VASCULAR PATTERN.”
Ultrasound Imaging: Sound waves can also be used to examine the inside of the eye. Ultrasound images of a choroidal hemangioma reveals that they are “bright.”This is because they are a mass of relatively large and well-formed blood vessels. Each blood vessel reflects sound waves producing characteristically intense reflections or moderately “MODERATELY HIGH INTERNAL REFLECTIVITY” from within the hemangioma tumor. Moderately high internal reflectivity is an important diagnostic characteristic.
Choroidal Hemangioma high internal reflectivity
Treatments
When a choroidal hemangioma is not causing symptoms, leaking or damaging the eye; it can be photographed and followed for evidence of change prior to treatment. However, if the choroidal hemangioma is documented to grow into the center of vision or is causing a retinal detachment or angle-closure glaucoma it is treated to save vision.
Hot Laser: Laser photocoagulation had been used to decrease the amount of fluid leaking out of choroidal hemangioma. Unfortunately, laser results are usually temporary and recurrence of retinal detachment or cystoid retinal degeneration usually results vision loss.
Photodynamic Therapy (PDT) is a cold or non-thermal laser treatment that involves injecting a light-sensitive dye into the patient and then shining a dye-activating PDT laser light on the choroidal hemangioma. The light-activated dye causes the abnormal blood vessels to close, shrink, and stop leaking. However, PDT requires that the tumor can be visualized during treatment. So, PDT will not work if there is a large retinal detachment covering the tumor or if the tumor is located too far anterior inside the eye. When it works, PDT offers a more long-term method to treat leaking posterior choroidal hemangiomas. The dye is expensive and multiple treatments are usually required. Lastly, due to changes in treatment patterns for AMD, fewer and fewer PDT laser machines and experienced PDT-laser surgeons exist.
Radiation Therapy: At The New York Eye Cancer Center most patients are treated with low-dose external beam or implant radiation therapy. Radiation has been used used to treat leaking choroidal hemangiomas for decades. The differences are, that in the past relatively large doses of radiation were used and some collateral radiation damage occurred. However, modern radiation techniques involve much lower doses of radiation as well as implant techniques that better focus the treatment area. Low dose radiation typically requires a total of less than two weeks of daily treatments. In Dr. Fingers’ experience, almost all choroidal hemangiomas and their associated retinal detachments can be cured with low dose radiation therapy.
Summary
Choroidal Hemangioma are benign tumors made up of blood vessels. Since choroidal hemangioma do not metastasize (spread to other parts of the body), we are more concerned with damage they can cause within the eye. Choroidal hemangioma can be stable and not require treatment. Others can change a patient’s vision by displacing the retina causing hyperopia (far-sightedness), causing degeneration of the overlying retina (cystoid degeneration), or by leaking fluid under and detaching the retina (serous retinal detachment).
Most choroidal hemangioma are treated if they induce a retinal detachment. Also in rare cases, choroidal hemangioma can fill most of the eye, affect the iris or be associated with the Sturge-Weber Syndrome. In these cases, the choroidal hemangioma (due to its increasing thickness) can cause angle closure glaucoma. In these cases, radiation can be used to cause regression and thinning of the hemangioma in the iris and prevent vision loss.
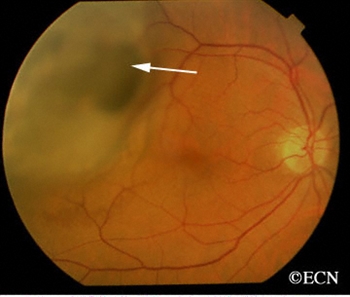
Malignant tumors from other parts of the body can spread in and around the eye. These tumors may never be discovered unless they affect vision, are visible to the patient, or push the eye forward. The most common location for ocular metastasis, in the vascular layer called the choroid (choroidal metastasis) within the eye.
Cancer metastasis that appear in and around the eye are usually from a breast cancer (in women) and lung cancer (in men). Other less common sites of origin include the prostate, the kidney, the thyroid, and gastrointestinal tract. Blood cell cancer (lymphoma and leukemia) can also metastasize to the eye and orbit. Once a patient is diagnosed with choroidal metastasis, we try to find where it came from. In 18% of patients, we do not find the source of choroidal metastasis. In these cases, we may have to biopsy the ocular tumor and look at its cell-type.
A small choroidal breast metastasis, the larger tumor was in the other eye.
Symptoms
Most patients with choroidal metastasis have no symptoms. If the metastasis is on the eye or eyelids, it may be visible. If located behind the eye (in the orbit), the metastasis can push the eyeball out or to the side. If within the eye (the most common), choroidal metastasis patients can see flashing lights, floating spots or distortion of their vision. Patients with a history of cancer are at greatest risk and should have periodic eye examinations.
Diagnosis
Most patients with metastasis have either a known primary cancer and/or metastatic tumors in other parts of their body. A careful medical history can uncover the signs or symptoms of these other cancers. If an eye cancer specialist suspects ocular metastasis, both eyes and orbits should be examined because ocular metastases can be both bilateral and/or multifocal.
Choroidal metastasis is usually non-pigmented (except metastatic melanomas), and has typical ultrasound and angiographic patterns. Choroidal metastasis is usually poorly circumscribed and can cause retinal detachments. They may have spicules of pigment on their surface. Unlike primary choroidal melanoma, they can grow quickly (weeks) and may require prompt treatment.
The patient with metastasis to the eye should also be examined by a medical oncologist. A complete metastatic survey should be performed to “stage” the patient (to see if there are other tumors within the body). Specifically, computed radiographic imaging of the brain and lung should be performed due to a high concurrent incidence of intracranial and pulmonary metastases. Your doctor may suggest a total body PET/CT with fusion.
Treatments
The care of patients with metastasis to the eye typically involves cooperation between the eye cancer specialist, medical oncologist, and radiation therapist. Though chemotherapy can be used in many cases of orbital and choroidal metastasis, radiation therapy is usually a more definitive treatment. If the metastatic tumor has not destroyed the center of the retina, early treatment offers the best hope for preserving vision. Almost all patients with choroidal metastasis can be treated with external beam radiation. That is, surgery is rarely needed as treatment for choroidal metastasis. Orbital and adnexal ocular metastasis are typically biopsied prior to treatment.
After irradiation, a regressed choroidal metastasis displays spicular hypertrophy of the retinal pigment epithelium.
Most patients who develop posterior choroidal metastasis can either be closely monitored for tumor growth, followed for response to chemotherapy, or treated with external beam irradiation. Radioactive plaque radiotherapy is rarely needed. If chemotherapy is not an option, prompt external beam irradiation (typically 30-40 Gy), may offer the best chance for preservation of vision.
In those rare cases where the metastasis spreads to the iris, patients can develop severe glaucoma and may lose their eye. Thankfully, anterior segment (iris) metastases are rare. Since most cancers do not spread to the iris, most patients with intraocular, choroidal and orbital metastasis respond well to treatment and keep their vision.
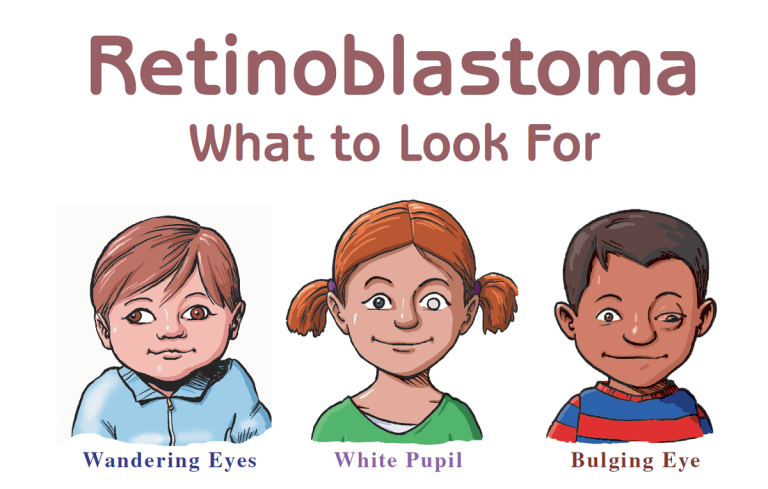
As a parent, you should trust your instincts. If you sense something might be wrong, you’re probably right. Ignoring your gut feeling could lead to tragic consequences.
Timely diagnosis is key to treating eye cancer. When caught early, doctors can often remove the tumor and preserve sight. But waiting too long can lead to loss of an eye or even death.
A British mother learned the consequences of delayed diagnosis the hard way.
“Ezmai had a lazy eye and we spoke to a health visitor and then took her to the pre-school vision team but they told me to come back in six months. I kept taking her but they couldn’t find anything wrong. My instincts told me there was something wrong with Ezmai but I felt no-one believed me and that I was going mad.”
Beasley said she took Ezmai to four different health care providers, but the child was not diagnosed with retinoblastoma until she was two. By then, the cancer had advanced to the point that surgeons had to remove her eye in order to save her life.
Beasley has now teamed up with the The Childhood Eye Cancer Trust in Great Britain to raise awareness of the importance of early diagnosis of retinoblastoma. According to the organization, 21% of children diagnosed with this rare form of cancer in 2015 experienced a delay of at least six months between their first visit to a general practitioner and examination by a specialist.
“We looked back at an old photo of Ezmai at Christmas in 2014 and we can see a white glow in her eye but at the time we had absolutely no idea this could mean she had cancer,” Beasley said.
The Eye Cancer Foundation offers a free-downloadable retinoblastoma poster and a program, and sponsors a program to teach fellows to become retinoblastoma specialists in unserved and underserved countries. Dr. Paul Finger said it is imperative to make medical professionals more aware of the symptoms.
“Clearly, early detection and prompt treatment of children with retinoblastoma is crucial for saving both their vision and life.”
If you notice any of unusual symptoms in your children, you should have them examined by a specialist as soon as possible. Trust your instincts and don’t allow doctors who are not trained in detecting eye cancer dissuade you from getting an examination by a specialist.
This is definitely a situation where you would rather be safe than sorry.
Uveal melanoma is a cancer of the eye involving the iris, the muscle surrounding the lens, or the choroid – a vascular layer with connective tissue between the retina and the sclera. It is a rare form of eye cancer with no effective therapies once it spreads to other parts of the body.
Uveal melanoma is related to more common cutaneous (skin) melanoma. Doctors have had success treating skin cancers with immunotherapies that boost naturally existing anti-tumor T-cell responses. In essence, this approach boosts the body’s natural immune system response to fight the tumor.
For instance, a drug called Keytruda was used to successfully treat Jimmy Carter’s melanoma. But despite the success of immunotherapy in attacking more common skin cancer tumors after it spreads, the role of this type of treatment for metastatic uveal melanoma remains unclear.
Fifteen researchers from the National Cancer Institute and other institutions embarked on a study to determine if this type of anti-tumor immune response exists against uveal melanoma.
To conduct the study, researchers surgically procured metastases from the livers of eye cancer and skin cancer patients. They then compared the tumor cell structures along with their associated T-cells using a variety of techniques.
Researchers found that despite the fact both are related to melanoma, the tumor cells differed in melanin content, the antigens provoking an immune response, and in their genetic mutations. The T-cells attacking the tumors were also different. Researchers found that anti-tumor T-cells in cutaneous melanoma were predominantly CD8+ while those in uveal melanoma were CD4+ dominant.
While the effectiveness of T-cells against the tumors was much higher in cutaneous melanoma, researchers found a subset of T-cells in uveal melanoma that had robust anti-tumor reactivity, comparable in magnitude.
Researchers say the absence of melanin pigmentation in the original tumor, before it metastasized to the liver, strongly correlated with the production of highly effective T-cells. In other words, a group of uveal melanoma tumors with lower melanin levels do seem to produce a promising immune system response that attacks the tumor
Knowing that a subset of uveal melanoma tumors with the ability to provoke an immune response exists opens the door to further research. Doctors can build on this knowledge to potentially discover therapies that will boost anti-tumor T-cell production and/or effectiveness to successfully treat this form of eye cancer even after it spreads..
In addition to his daily work treating his own patients at the NYECC, Dr. Finger is committed to advancing research that will benefit people diagnosed with eye cancer around the world.
In that spirit, Dr. Finger is working with the Ophthalmic Oncology Task Force to create a database on vitreoretinal lymphoma that will ultimately lead to more effective treatments and better patient outcomes.
Primary vitreoretinal lymphoma (PVRL) is a variant of central nervous system lymphoma with initial or primary manifestation in the eyes. It is a typically aggressive, diffuse large B-cell malignancy. Patients diagnosed with PVRL generally have a poor prognosis.
Currently, there is very little evidence-based, statistically significant information about vitreoretinal lymphoma. To gather this vital data, Dr. Finger and the Ophthalmic Oncology Task Force have create an International Vitreoretinal Lymphoma Tumor Registry.
Information gathered through the registry will help determine the best local and systemic treatment strategies. Because vitreoretinal lymphoma is often associated with central nervous system lymphoma, this information will help save both vision and life.
The goal is to register 2,500 cases of vitreoretinal lymphoma in the database from participating centers around the world. Each center must be able to enroll at least 50 cases diagnosed between the years 2000 to 2015.
The database will anonymize patient information and conform to all privacy standards. All data mining related publications will include two authors from each center. Though there will be a group authorship as primary, each center will be listed in order, according to the number of patients entered into the database.
The ultimate success of the Vitreoretinal Lymphoma Tumor Registry will depend on the participation of retinal specialist, ophthalmic oncologist, and hematologist oncologist. If you are a physician specializing in these areas and you’re interested in participating in the registry, please contact Dr. Finger at pfinger [at] eyecancer [dot] com.
Your smartphone camera flash can detect a rare eye cancer, potentially saving a child’s life.
That was the case for an Arizona mother who inadvertently detected retinoblastoma in her young son after using a flash phone camera to take pictures of him. Andrea Temarantz noticed a white glow in the left eye of her son Ryder in the photographs she’d taken. Suspecting it was due to a faulty phone camera, Temarantz switched to a better device. When the white spot remained, she took Ryder to see a doctor. The physician identified a tumor, and diagnosed him with retinoblastoma, a potentially fatal eye cancer.
While rare, retinoblastoma is a very aggressive eye cancer found almost exclusively in young children. Leukocoria (white pupil) and misaligned eyes (strabismus) are the most common symptoms. In other cases, the child may have developed neovascular glaucoma and may be in pain. Retinoblastoma treatment typically requires the cooperation of an ophthalmic oncologist, pediatric oncologist, and radiation therapist. Over the last 30 years, treatment has evolved from enucleation (removal of the eye), to eye-sparing radiotherapy. More recently doctors have treated selected patients with chemotherapy-based multi-modality therapy.
An early diagnosis is critically important for successful treatment. Retinoblastoma is almost always fatal when left untreated.
When flash photography creates a white pupil in the eye of a child, it could be that the light is illuminating a tumor not otherwise visible. While a white spot in the eye is not always indicative of a tumor, a visit to the doctor for a diagnosis is always a good precautionary measure.
Temarantz’s experience was not an isolated case. A Rockford, Illinois, child owes his life to a camera flash and a vigilant parent. Julie Fitzgerald noticed a white spot in showing up in photos of her son Avery’s left eye. After reading stories online about similar cases, she decided to take her son to see a doctor. Avery was ultimately diagnosed with retinoblastoma. Unfortunately, his left eye had to be removed, but the diagnosis saved his life.
Using a smartphone’s camera flash to detect a potential instance of retinoblastoma is effective enough that the UK-based Childhood Eye Cancer Trust conducted an ad campaign in 2014 to raise awareness of its life-saving potential for early detection.
A drug thrust into the limelight by Jimmy Carter shows promise for treating melanoma of the eyelid.
Keytruda (pembrolizumab) gained FDA approval for limited treatment of metastatic melanomas in late 2014. The agency gave its blessing for front-line treatment in patients with unresectable or metastatic melanoma on Jan. 7 of this year.
The drug is a form of immunotherapy and works by unleashing the body’s immune system to attack cancerous melanin cells. If the cancer is not caught early, it can spread deep into the skin and spread to other organs. At that point, chemotherapy becomes generally ineffective. Testing has shown Keytruda can drastically increase survival rates for advanced skin cancer.
Keytruda is what is known as a PD-1 inhibitor. T-lymphocyte cells are the body’s primary cancer fighter. Tumors express proteins called PD-L1 and PD-L2. These “program death” proteins lure T-lymphocyte cells to bind to them. Eventually, this results in T-cell exhaustion and reduces their ability to fight the cancer. Keytruda works by targeting the PD-1 receptors, allowing the body’s immune system fight the cancer cells. UConn doctors say they have had great success using Keytruda, according to Dr. Upendra P. Hegde, an associate professor in the Department of Medicine.
“Keytruda is the first PD-1 inhibitor drug that is allowing us to shrink the melanoma tumors in up to 35 percent of our UConn Health patients, and we are continuing to see more progress over time.”
“The study…tested Keytruda against Yervoy in more than 830 patients whose melanoma had spread to other parts of the body. About one-third of patients received Keytruda once every two weeks, one-third received it every three weeks, and the remaining one-third received the standard four cycles of Yervoy. One year after the start of treatment, 74% of patients who received Keytruda every two weeks and 68% of those who received it every three weeks were still alive, compared with 58% for those who received Yervoy. Measured another way, Keytruda reduced the risk of death by 31% to 37% versus Yervoy, according to the results, which were published online Sunday by the New England Journal of Medicine and presented at the annual meeting of the American Association for Cancer Research in Philadelphia.”
A similar drug approved for melanoma treatment has shown similar promise. Opdivo (nivolumab) works in the same way as Keytruda, blocking the PD-1 receptors. A study presented at the 2015 Society for Melanoma Research Congress showed the 2-year overall survival rate with frontline nivolumab was 57.7%.
Jimmy Carter underwent treatment for his melanoma with Keytruda. He was diagnosed with an aggressive form of skin cancer that had spread to his brain and liver. In December, the former president announced he was cancer-free, putting the cancer-fighting drug in the national spotlight.
"Very well treated by Dr. Finger. He explained everything I needed to know about my issue with detail and attention, putting me at ease and giving me confidence to handle this problem for the rest of my life.”
– N.N.